

Glossopharyngeal neuralgia (GPN) is a rare type of headache presenting as paroxysmal electrical shock-like pain affecting the tongue, soft palate and pharynx, the areas innervated by the somatosensory branches of glossopharyngeal and vagus cranial nerves [1-3]. Symptoms are provoked by swallowing, coughing, yawning, or talking, and can be associated with syncope, bradycardia, hypotension, or even asystole, by spillover of the neural excitation to the parasympathetic dorsal motor nucleus of the vagus nerve [1-3]. The compression of the nerve root by the adjacent vessels such as posterior inferior cerebellar artery (PICA), vertebral artery (VA), veins, or their combination, accounts for the most cases of GPN [4,5]. In this case, we report that GPN is attributed to the traction, mild displacement and compression of the glossopharyngeal nerve by tortuous VA and proximal PICA. Furthermore, we demonstrate the effective outcomes of medical treatment in managing this condition.
CASE
A 74-year-old woman with hypertension and hyperlipidemia, and no comorbid headaches, presented with intermittent severe lancinating pain in the base of her tongue, the left side of the soft palate, and the left side of the pharynx, which was developed 6 months prior to her hospital visit. This pain was mainly provoked by swallowing food or yawning, and its frequency and severity was slowly increasing over the 6 months. Although the precise frequency was not recorded, she mentioned that initially the frequency was less than ten episodes per day, but it progressively increased to nearly 100 times per day. The neurological examination revealed no abnormality, except for the decreased facial sensation in the V1 division of the left trigeminal nerve, probably due to the prior history of herpes zoster infection in that area.
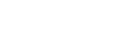
Magnetic resonance angiography revealed a left PICA originating from the tortuous left VA and descending with an acute angle (Fig. A). In high-resolution axial T2 magnetic resonance image of brain (Fig. B-D), left glossopharyngeal nerve was compressed and slightly displaced to the inferolateral side by the angle between VA and PICA origin. Diagnostic digital subtraction angiography was performed for the evaluation of the incidentally found anterior cerebral artery aneurysm, which confirmed the tortuosity of the V4 segment of the left VA and left PICA, making an acute angle between those arteries (Fig. E, F). She was initially prescribed with 100 mg of carbamazepine twice a day, and after 1 week of medication, the frequency of pain was unchanged, but the severity of the pain decreased by 20% compared to before starting the medication. After the dosage was increased from 100 to 200 mg twice a day, she experienced a sense of fuzziness, dizziness, and unsteadiness. Consequently, the dosage was reduced back to the initial level. Given that the patient was reluctant to the surgical intervention, gabapentin (100 mg, three times a day) was combined to carbamazepine, which achieved an 80% reduction in the frequency and the severity of pain.
CONCLUSION
This is an illustrative case of GPN that is caused by the tortuous VA and proximal PICA tugging down and compressing glossopharyngeal nerve as PICA originates from VA with an acute angle. Along with the high anatomical variability in the location of origination and the course of PICA [6], the high susceptibility of VA for the aging-related progression of vascular tortuosity might be the possible explanations for the progressive aggravation of symptoms in this case [7]. Although microvascular decompression with or without nerve dissection is treatment with high safety and long-term efficacy [3-5,8], medical treatments including carbamazepine, gabapentin, pregabalin, and analgesics can also be effective, even in the cases with overt compression and traction of glossopharyngeal nerve as in this case [1-5].
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




