

서 론
가족성 고콜레스테롤혈증(familial hypercholesterolemia, FH)은 상염색체우성유전질환으로 대개 저밀도지질단백(low-density lipoprotein, LDL)수용체의 부족이나 결함으로 인한 지질단백의 대사장애를 초래하는 선천 질환이다[1]. 가족성 고콜레스테롤혈증은 정상인보다 2-4배 높은 LDL콜레스테롤 수치를 보이는데, 이 중 이종접합(heterozygous) 형태의 가족성 고콜레스테롤혈증은 hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) 환원효소억제제(reductase inhibitor)로 치료할 수 있으나 동종접합(homozygous) 형태의 경우는 약물 치료 시의 반응이 좋지 않아 질병을 조절하기가 어렵다[1]. 그 유병률은 약 500-1,000명당 1명꼴이고, 국내에는 약 10만 명의 환자가 있을 것으로 추정한다[1]. 가족성 고콜레스테롤혈증의 진단은 환자나 가족 중에 저밀도지질단백이 비정상적으로 상승해 있거나 신체검진상 힘줄황색종(tendon xanthoma) 또는 각막환(arcus cornealis)이 있는 경우, 50-60세 이전에 심근경색을 앓은 가족력이 있는 경우 질환을 의심해볼 수 있고, 이 때 임상양상, 콜레스테롤 수치 그리고 유전자검사를 포함한 각종 진단기준을 적용하여 진단에 이르게 된다[1]. 가족성 고콜레스테롤혈증 환자는 유년기부터 콜레스테롤 수치가 매우 높기 때문에 30세 이전에 급성관상동맥허혈증상이나 심근경색을 유발하여 급사할 수 있고 따라서 적극적인 지질강하치료가 필요하다[1].
혈중의 콜레스테롤의 극심한 증가는 전신 혈관의 동맥경화 반응을 가속화시킴으로서 관상동맥뿐 아니라 뇌혈관 사건 역시 높이리라 예상되나 아직까지 국내에서 가족성 고콜레스테롤혈증과 관련된 뇌졸중에 대한 보고는 없다[2]. 이는 뇌동맥은 관상동맥보다 가족성 고콜레스테롤혈증의 병리기전에 영향을 덜 받아서 그럴 수 있겠으나 뇌경색 환자를 진료하는 의료진의 가족성 고콜레스테롤혈증에 대한 인식 부족으로 충분한 평가가 이루어지지 않아 질병의 진단을 받지 못할 가능성도 있다[3]. 따라서 저자들은 뇌경색 환자들 중 가족성 고콜레스테롤혈증이 의심되는 환자들을 선별하여 이들의 임상양상과 뇌경색의 발생기전 그리고 치료 전후의 LDL콜레스테롤 수치와 적절한 치료를 받고 있는지 여부를 알아보고자 한다.
대상과 방법
2014년 1월부터 2017년 5월까지 중앙대학교병원에 입원하였던 뇌경색 또는 일과성허혈발작 환자들 중에서 Dutch Lipid Clinic Network Diagnostic Criteria (Table 1) [3]을 적용하여 가족성 고콜레스테롤혈증이 의심되는 환자들을 선별하였다. 해당 진단기준은 1) 조기 심혈관질환 가족력 또는 LDL콜레스테롤 95 percentile 이상 가족력, 조기 관상동맥질환, 2) 조기 뇌혈관질환 또는 말초혈관질환 과거력, 3) 힘줄황색종 또는 각막환 같은 신체검진상의 소견, 4) LDL콜레스테롤 수치 그리고 5) low-density lipoprotein receptor (LDLR), apolipoprotein B (Apo B) 또는 proprotein convertase subtilisin/kexin type 9 (PCSK9)유전자 돌연변이 유무 5가지 항목으로 구성되어 각각의 항목 점수를 통합하여 definite/probable/possible/unlikely로 가족성 고콜레스테롤혈증 진단 여부를 결정하게 된다[3]. 연구진은 가족성 고콜레스테롤혈증이 의심되는 환자의 동반 혈관 위험인자 및 가족력 그리고 입원 당시 시행한 뇌영상검사 및 혈액검사 결과는 뇌졸중 레지스트리를 이용하여 수집하였다. 뇌경색의 기전은 내원 당시 시행한 뇌영상검사 및 심장검사 결과를 바탕으로 Trial of Org 10172 체계를 적용하여 분류하였다[4]. 환자들의 지질강하약제의 종류 및 용량, 퇴원 시 신경계 상태, 퇴원 후 뇌졸중 재발 여부에 대한 정보는 의무기록을 통하여 수집하였다.
결 과
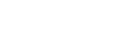
해당 기간 동안 총 1,401명의 뇌졸중 환자가 뇌졸중 레지스트리에 등록되었고 이 중에서 4명(probable FH 1명, possible FH 3명)의 가족성 고콜레스테롤혈증 의심 환자가 확인되었다(Fig. 1). 이들은 모두 남자였으며 과거 관상동맥질환은 없었고 뇌경색 발병 당시 연령은 3명은 30대이고 나머지 1명은 50세였다(Table 2). 한 명의 환자를 제외한 환자는 정기적인 외래 추적관찰 및 혈액검사를 최소 2년 이상 유지하였으며 뇌졸중을 포함한 혈관 사건의 재발은 없었다. 네 명의 환자들의 지질 수치는 일반 뇌경색 환자보다 약 두 배 가량 월등히 높았다(총콜레스테롤: 일반 뇌경색군 178±47 mg/dL, FH군 378±75 mg/dL; LDL콜레스테롤: 일반 뇌경색군 105±34 mg/dL, FH군 238±56 mg/dL). 모든 환자에서 magnetic resonance imaging (MRI) 또는 computed tomography (CT)를 통한 뇌혈관 평가에서 중등도 이상의 협착이 동반되어 있었는데 두 명은 동맥경화성, 나머지 두 명은 혈관박리에 의한 협착으로 추정되었다. 네 건의 뇌경색의 간략한 임상적인 특징은 다음과 같다(Fig. 2).
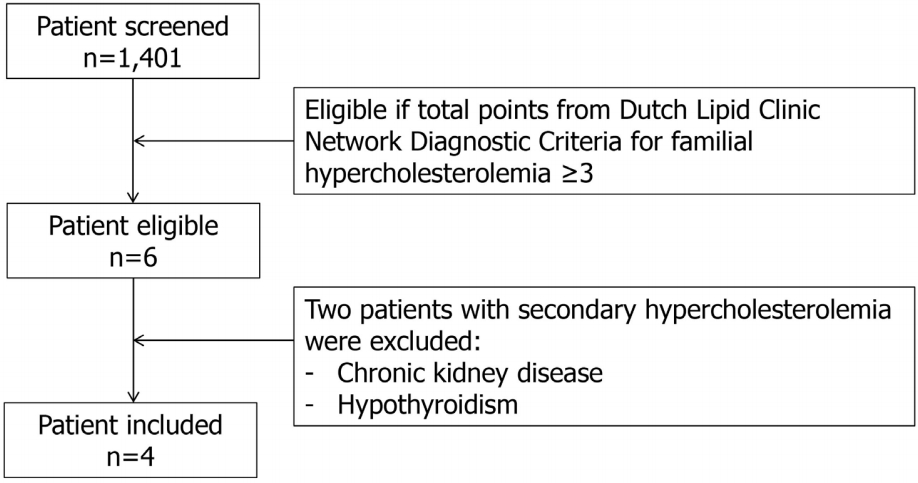
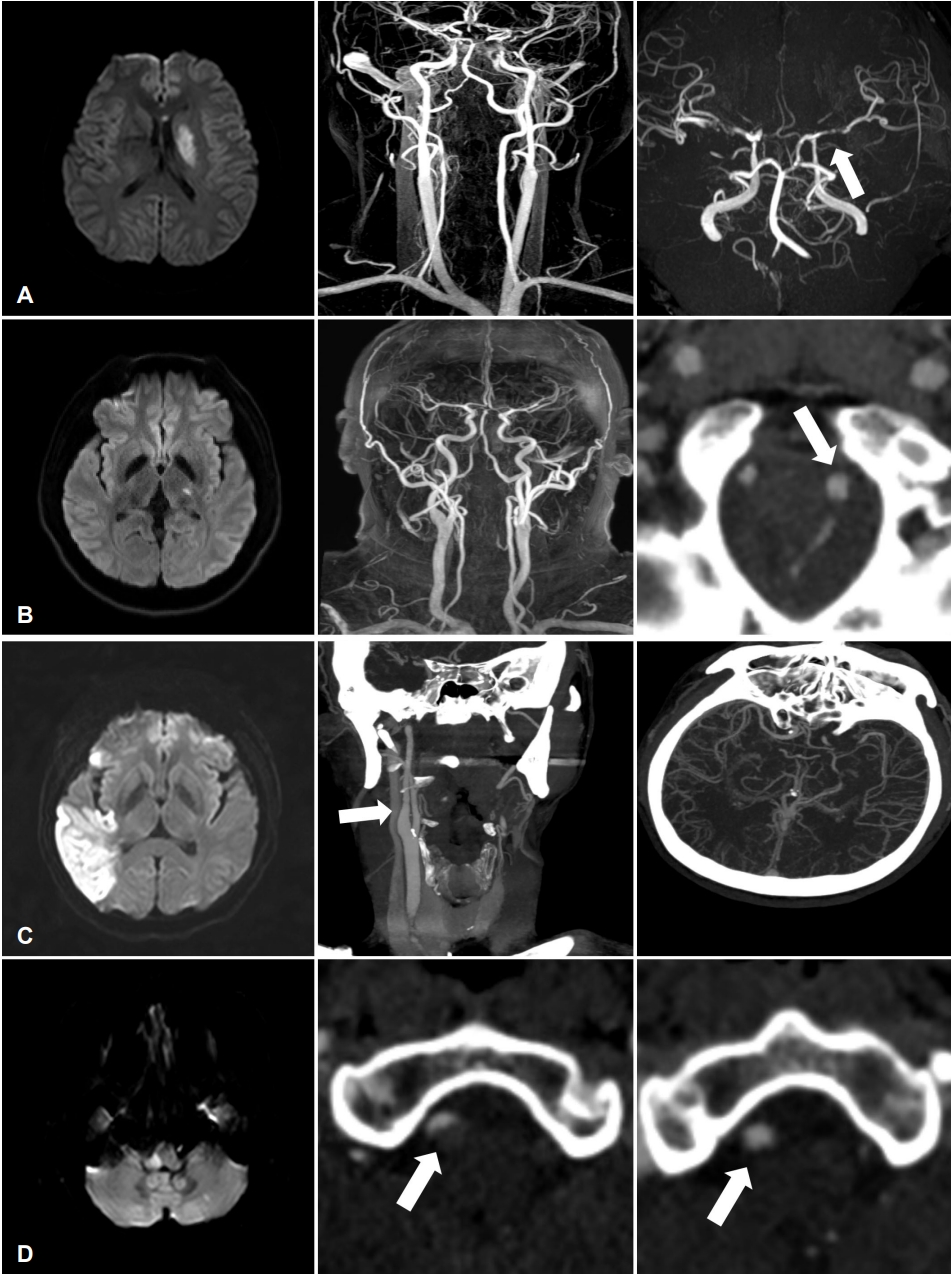
첫 번째 환자는 34세 남성으로 갑자기 발생한 우측 안면마비와 구음장애를 주소로 내원하였다. 뇌 MRI 결과 왼쪽 방사관(corona radiata)에 급성 뇌경색이 있었고, 좌측 중대뇌동맥이 거의 막혀 있었다(Fig. 2-A). 뇌경색 발병기전은 대혈관 죽상경화로 진단하고 초기 LDL콜레스테롤 수치는 196 mg/dL였다. 뇌경색 진단 이후 아스피린 100 mg, clopidogrel 75 mg, pravastatin 40 mg을 복용하기 시작하였고 퇴원 시 신경계 후유증 없이 퇴원하였다. 퇴원 2주 후 외래에 내원하였을 때 비특이적인 어지럼증과 구음장애를 호소하여 뇌 MRI를 다시 시행하였으나 뇌경색 재발은 없었다. 1년 후 뇌혈관조영검사를 시행하여 모야모야병(moyamoya disease)도 의심하면서 외래 추적관찰을 유지하고 있다. 이후 4년간 지질강하치료를 지속하는 중으로 최종 혈액검사에서 LDL콜레스테롤은 127 mg/dL로 확인되었다.
두 번째 환자는 37세 남성으로 갑자기 발생한 우측 상하지 감각 저하를 주소로 내원하였고 고혈압 및 흡연력이 있었다. 뇌 MRI에서 좌측시상(thalamus)에 뇌경색이 있었고 혈관영상검사에서 좌측 추골동맥의 박리 소견이 있었다(Fig. 2-B). 내원 당시 LDL콜레스테롤 수치는 196 mg/dL였고, 뇌경색 기전은 기타(other determined), 즉 혈관박리에 의한 것으로 생각하였고 아스피린 100 mg과 atorvastatin 80 mg을 복용하였다. 환자는 퇴원 전 시행한 혈액검사에서 LDL콜레스테롤 수치는 122 mg/dL로 감소하는 경향을 확인하였으나 퇴원 후 외래를 방문하지 않아 혈관 사건 재발 여부는 알 수 없었다.
세 번째 환자는 50세 남성으로 갑자기 발생한 의식저하 및 전신경직을 주소로 내원하였고 뇌 MRI를 통하여 우측 중대뇌동맥 영역의 급성 뇌경색을 진단하였다. 혈관영상검사에서 우측 중대뇌동맥의 부분 협착과 우측 전대뇌동맥의 폐색을 확인하였다(Fig. 2-C). 혈액검사에서 C단백활성(protein C activity) 170% (정상: 70-130%), 보체C4 (complement C4) 43.4 mg/dL (정상: 10-40 mg/dL), 섬유소원(fibrinogen) 754 mg/dL (정상: 140-400 mg/dL), anti-beta 2-glycoprotein I (GPI) immunoglobulin (Ig) M 22.0 units (정상: 0-20 units)로 상승되었고, 숨겨진 악성 종양 여부를 확인하고자 시행한 복부 CT에서 우측 신장 경색을 추가로 발견하였다. 이에 뇌경색의 기전은 기타-응고장애에 따른 것으로 의심하고 와파린으로 항응고 치료를 유지하였다. 초기 LDL콜레스테롤 수치는 314 mg/dL로 높았으나 atorvastatin 40 mg을 유지하였고 3년 후 추적검사에서는 91 mg/dL로 확인되었다. 이후 anti-beta 2-GPI IgM 재검사는 시행하지 않아 항인지질항체증후군 확진에 이르지는 못하였다.
네 번째 환자는 38세 남성으로 갑자기 발생한 어지럼증과 구음장애로 내원하였으며 뒤통수 부위에 두통을 동반하였다. 뇌 MRI에서는 우측 가쪽 연수와 좌측 소뇌를 침범하는 뇌경색이 발견되었다. 뇌 CT혈관조영술에서 우측 추골동맥 박리가 확인되어 뇌경색의 기전은 기타-혈관박리로 진단하고 아스피린 100 mg, cilostazol 200 mg을 처방하였다(Fig. 2-D). 초기 LDL콜레스테롤 수치는 246 mg/dL로 확인되었으며 pitavastatin 2 mg 처방을 유지하였고, 2년 후 LDL콜레스테롤 수치는 92 mg/dL로 확인하였다. 1년 후 뇌 CT혈관조영술에서 우측 추골동맥 박리는 회복되었다. 본 연구가 후향적으로 진행됨에 따라 환자들을 검진할 당시 가족성 고콜레스테롤혈증과 관련된 가족력, 신체검진에서의 이상 여부, Apo B 또는 PCSK9유전자 변이와 같은 임상 정보는 확인하지 못하였다.
고 찰
본 연구는 가족성 고콜레스테롤혈증이 동반된 뇌경색 환자의 뇌경색 발병기전 및 예후에 관한 최초의 보고이다. 이번 연구는 단일 기관 뇌졸중 레지스트리에 등록된 환자 중에서 가족성 고콜레스테롤혈증 진단기준을 적용하여 의심 환자를 발굴하였고 그들의 뇌경색 특성과 기전을 기술하였다. 그 결과 환자들은 다양한 수준의 뇌혈관 죽상경화가 동반되어 있었으나 뇌경색의 기전이 죽상경화에 의할 것이라는 가설과는 달리 혈관박리, 응고체계교란 등 다양함을 확인하였다.
가족성 고콜레스테롤혈증 환자에서 관상동맥질환 등 혈관 사건 발병률이 일반 인구보다 약 10배 가량 높다고 알려져 있기 때문에 상기 질환이 의심되는 경우 유전자검사를 포함한 적절한 평가 및 적극적인 지질강하치료를 고려해야 한다[1]. 본 연구에서는 1,401명의 뇌경색 환자 중에서 가족성 고콜레스테롤혈증이 의심되는 환자 4명이 발견되었으나 그 유병률은 약 0.3% 수준으로 일반적으로 알려진 0.1-0.2%를 조금 웃도는 수준이다. 가족성 고콜레스테롤혈증이 뇌졸중 발병 위험성을 높이는지에 대해서는 다양한 연구 결과가 존재하며, 최근 북유럽에서 진행된 대규모 유전체 분석 기반 코호트 연구에서는 뇌졸중 발병과는 뚜렷한 상관관계는 없음을 보고하기도 하였다[5,6]. 국내에서 한국지질동맥경화학회가 주축이 되어 진행한 가족성 고콜레스테롤혈증 환자 등록 사업 결과에서도 약 97명의 환자 중에서 혈관 사건을 경험한 환자는 관상동맥질환을 동반한 환자가 27명이고 뇌졸중 환자는 한 명도 없었다[2]. 가족성 고콜레스테롤혈증이 관상동맥질환 발병보다 뇌졸중 발병과의 연관성이 떨어지는 이유는 뇌졸중은 죽상경화 이외의 기전, 즉 심방세동, 뇌소혈관질환 그리고 뇌출혈 등 다양한 기전으로 발병할 수 있어 고콜레스테롤혈증이 기여하는 바가 희석되리라 예상한다. 또한 최근 스타틴의 적극적인 처방으로 가족성 고콜레스테롤혈증과 뇌졸중과의 관련성이 약화되었다고 분석하는 연구 결과도 존재한다[7]. 그럼에도 본 연구에서는 가족성 고콜레스테롤혈증 의심 환자에서 다양한 기전에 의한 뇌경색이 확인되었는데, 이는 가족성 고콜레스테롤혈증의 혈중 콜레스테롤 상승이 뇌혈관의 죽상경화 반응을 초래할 뿐만 아니라 혈관 내막 손상에 따른 동맥박리 및 혈액응고체계 교란 등 다양한 기전으로 뇌혈관 사건을 유발할 수 있음을 시사한다. 실제로 혈액응고체계에 대한 연구에서는 가족성 고콜레스테롤혈증으로 진단받은 환자의 혈액에서 진단받지 않은 가족 구성원보다 응고인자VIII이 약 9% 가량 유의하게 상승되어 있음이 밝혀졌다[8].
가족성 고콜레스테롤혈증 환자에게 가장 많이 처방되는 지질강하제는 HMG-CoA 환원효소억제제인 스타틴으로서, 체내 콜레스테롤 합성을 줄이면서 LDL수용체를 활성화시켜 혈중 LDL콜레스테롤 농도를 낮추는 것으로 알려져 있다[9]. 그러나 최근 국내 연구에 따르면 가족성 고콜레스테롤혈증 환자에서 적극적인 스타틴 처방에도 불구하고 목표 LDL콜레스테롤 수치에 도달하는 비율은 채 절반이 되지 않는 것으로 확인된다[9]. 스타틴 효과가 불충분한 경우 ezetimibe, 담즙산결합수지 그리고 니코틴산 등 다른 기전의 약제를 함께 처방하면 추가적인 LDL콜레스테롤 강하 효과를 예상할 수 있다[1]. 본 연구에서 확인된 모든 환자가 다양한 종류의 스타틴 처방을 받았는데 두 명의 환자만이 고강도 스타틴 처방을 유지하였음에도 초기 LDL콜레스테롤 수치 대비 약 35-70% 감소 효과를 보임으로서 대부분의 환자들에서 지질강하 효과는 비교적 우수하였다. 만약 경구 투여로 만족할 만한 지질강하 효과를 보이지 않는 경우에는 최근 부상하고 있는 단일클론항체 기반의 PCSK9억제제 또는 RiboNucleic Acid상보서열에 의한 Apo B antisense인 mipomersen 처방을 고려할 수 있다[1]. 대표적인 PCSK9억제제인 에볼로쿠맙은 가족성 고콜레스테롤혈증 환자를 대상으로 진행된 대규모 임상 연구에서 LDL콜레스테롤 수치를 대조군 대비 약 55%까지 감소시키는 효과를 보인 바 있다[10].
본 연구의 주요 한계점은 가족성 고콜레스테롤혈증의 진단이 환자가 내원한 시점에 이루어진 것이 아니라 후향적으로 기록된 임상 정보와 지질 수치 등을 기반으로 이루어진 점이다. 따라서 주로 젊은 뇌졸중 발병 연령과 LDL콜레스테롤 수치만으로 가족성 고콜레스테롤혈증 진단이 이루어지고 진단에 중요한 가족력과 신체검진 소견에 대한 체계적인 정보 수집이 부족하여 다수의 의심 환자를 발견하지 못하였을 가능성이 높다. Table 1에 소개된 Dutch Lipid Clinic Network Diagnostic Criteria for FH에 따르면[3] 뇌졸중 과거력이 있는 55세 미만의 남성, 60세 미만의 여성은 1점이고, LDL-cholesterol (LDL-C) 범위에 따라 1, 3, 5, 8점이 추가된다. 따라서, 뇌졸중 레지스트리에 등록된 환자들 중 해당 연령대이면서 LDL-C 190 mg/dL 이상이라면 최소 total score 4점 이상으로 probable FH로 진단할 수 있는 조건을 만족하게 된다. 환자가 뇌졸중 발병 전 스타틴 치료를 받고 있는 경우에는 LDL콜레스테롤 수치가 낮아짐에 따라서 가족성 고콜레스테롤혈증의 진단이 내려지지 않은 가능성도 존재한다. 또한 유전자검사를 통하여 진단에 이른 환자는 한 명도 없었던 것도 한계점이다. 한국의 가족성 고콜레스테롤혈증 환자의 임상양상 연구에 의하면 혈중 LDL콜레스테롤 수치가 225 mg/dL 이상인 경우 병적인 유전자 이상을 의심해볼 수 있다[11]. 따라서 젊은 뇌경색 환자가 입원하였을 때 혈관 사건의 가족력이 있으면 신체검진에서 힘줄황색종이나 각막환 여부를 확인하고, LDL콜레스테롤이 225 mg/dL 이상으로 상승되어 있으면 LDLR유전자검사 등을 시도해볼 수 있다. 그러나 가족성 고콜레스테롤혈증과 관련된 유전자 이상은 잘 알려진 LDLR유전자뿐 아니라 Apo B 또는 PCSK9유전자 돌연변이도 있을 수 있고 그 밖에도 다양한 유전자 변이가 알려져 있다[11]. 가족성 고콜레스테롤혈증 진단이 이루어진 경우 가족 구성원에 대한 선별검사를 실시한다면 더 많은 사람에서 혈관 사건 발생을 예방할 수 있다.
본 연구는 가족성 고콜레스테롤혈증이 동반되어 있는 뇌경색 환자에서 뇌경색의 발병기전을 분석하고 지질강하치료제 처방 실태 및 그 효과를 파악하였다. 향후 전향적인 다기관 연구를 통하여 가족성 고콜레스테롤혈증에 따른 뇌경색의 보다 정확한 임상 특성과 효과적인 치료 전략을 수립하는 시도가 필요하다. 이를 통하여 뇌경색 환자에서 가족성 고콜레스테롤혈증을 적극적으로 진단하고 적절히 치료할 수 있는 근거를 마련할 수 있을 것이다.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print




