노인 보행의 특성: 정상과 비정상
Characteristics of Gait in the Elderly: Normal vs. Abnormal
Article information
Trans Abstract
Human gait inevitably deteriorates with “physiologic” aging as well as age-related pathologic conditions particularly in the older adults. However, some of them maintain relatively normal gait pattern well into their 80s. The existence of “successful aging” group in terms of gait performance suggests that senile gait is no more a consequence of aging alone. Here, we discuss age-related change of gait to characterize gait in the elderly, and briefly review the classification system of gait disorders in the elderly.
서 론
노인에서 비정상 보행은 매우 흔히 발견되고, 일반인의 단순한 관찰만으로도 쉽게 구별되는 것처럼 보이지만 실제로는 노인 정상 보행의 명확한 의학적 기준이나 협의된 정의가 없어 비정상 보행을 식별하기가 쉽지 않다. 노인 보행장애(gait disorder)의 유병률은 정확히 알려져 있지 않지만 지역사회 기반 연구에서는 60세 이후 15% 이상, 80세 이후로는 30%에 이르는 것으로 추정되며, 의료기관 및 요양시설 거주 노인 대상 연구에서는 이보다도 훨씬 높을 것으로 예상된다[1-4]. 이처럼 매우 높은 노인 보행장애 유병률을 고려하면, 노년기까지 정상 보행을 유지하는 것은 “성공적 노화(successful aging)”의 핵심 요소라고 할 수 있다. 따라서, 노인 비정상 보행을 확인하고, 그 원인에 따른 약물적 또는 중재적 치료와 지속적 운동 치료를 통해 보행기능을 개선시키는 일은 노인 의학에서 매우 중요한 분야의 하나로 생각된다. 이에 저자는 노화에 따른 보행 변화 양상을 임상 소견과 보행 분석 연구 결과를 토대로 기술하고, 노인 보행장애의 분류 체계를 통해 노인들의 비정상 보행 양상에 대하여 간략히 살펴보기로 한다.
본 론
1. 노화에 따른 보행 변화
인간의 보행은 일견 매우 단순한 반복 동작처럼 보이지만 실제로는 근골격계, 운동 및 감각 신경계, 심혈관계 그리고 환경 상호간의 매우 복잡한 기전에 의하여 직립 상태에서 양발의 디딤기(stance phase)와 흔듦기(swing phase)가 서로 교대로 진행되며 개체를 전방으로 이동시키는 일련의 율동적·주기적 반복 동작이다(Fig. 1)[5]. 보행주기의 시작은 관습적으로 신전된 무릎 쪽 발뒤꿈치로 지면을 딛는 시점으로 정의되며(heel strike), 주기의 60-65%의 기간은 한쪽 발바닥이 땅에 붙어 있는 디딤기이고, 나머지 35-40%의 기간 동안 발이 땅에서 떨어져 움직이는 흔듦기로 구성되는데, 전체 보행주기의 20-25%의 기간은 두 발이 모두 땅에 닿아 있는 양다리지지기(double limb support phase)에 해당된다. 이러한 보행주기의 각 요소는 보행 분석실에서 측정되며, 노화에 따라 점차 걸음의 속도가 느려지고, 보폭이 짧아지면서 보행주기의 흔듦기가 줄어들고, 두 발로 지탱하는 양다리지지기가 차지하는 비율은 늘어나게 된다.
Normal gait cycle.
출생 이후 신체 발달 및 신경계의 발달에 따라 완성된 직립 보행은 30세 이후 개개인의 유전적 배경과 환경적 요인에 의해 각기 다른 정도의 노화에 따른 영향을 받게 된다. 보행기능의 퇴행은 75-80세 이후 분명해지는데[6], 1931년 Critchely는 걸음 거리(stride length)가 짧아지고, 양발의 간격(stance width)은 약간 넓어지며, 유연성이 감소되고, 약간의 체위 불안정과 함께 다소 구부정한 자세, 발걸음의 크기가 작고(small steps), 전방돌진(propulsion) 성향을 보인다고 기술하고 이를 “노인 보행(senile gait)”으로 처음 명명하였다. 이후에도 노인 보행의 다양한 특성이 연구되었는데, 이러한 특징만으로 비정상 보행을 구분하기에는 모호함이 남는다[2,3].
최근에는 다양한 보행 분석 기술의 발달로 보행에 관련된 다양한 운동학(kinematic) 및 운동역학(kinetic) 변수들의 정량적 분석이 가능해졌으며 이를 통해 연령 증가에 따른 변화를 보다 객관적으로 평가하려는 시도가 이루어지고 있다. 보행 분석 연구 결과 건강한 80대 노인의 정상 보행 속도는 1.0-1.2 m/s 정도로 알려져 있는데, 이는 20대 건강한 대조군에 비해 10-20% 정도 감소되어 있는 정도이며, 걸음 간격(stride width)과 양발디딤기(double support time)가 경미하게 증가되어 있음이 확인되었다. 특히, 보행 속도의 경우 60세까지는 1% 미만의 매우 경미한 감소를 보이지만, 이후 80세까지는 매년 1-2% 정도의 감소 양상을 보인다[7]. 따라서, 보행 속도와 걸음 거리의 감소가 이러한 기준을 벗어날 정도로 매우 심하거나 특히 평형기능이 함께 손상되어 있는 경우라면 질병에 의한 보행 변화일 가능성이 단순히 연령에 의한 변화일 가능성보다 크다고 할 수 있다. 이처럼, 노화에 따른 보행 속도 감소는 걸음 거리의 감소에 따른 결과이며(보행률[cadence]은 비교적 일정하므로), 그 원인으로는 관절 경직도, 하지 근력 그리고 에너지 보존 전략의 경미한 변화 등이 추정되고 있다. 그 밖에도 보행 변이성(gait variability) 증가, 발목 가동 범위 감소, 골반 회전량 감소, 발뒤꿈치 디딤 시 발목 굽힘 정도의 감소, 흔듦기의 감소 등 노인 보행의 다양한 지표들의 경미한 변화가 보고되어 왔다[3,8,9]. 최근 신체부착형 센서(wearable sensor)를 이용한 지역사회 기반의 건강한 전 연령층 대상 연구를 통해 연령별 다양한 보행 관련 지표들의 정상 분포와 변화 양상이 조사되어 노인 보행을 보다 객관적으로 평가하는 데 도움이 되고 있다(Fig. 2)[10].
Age-related changes in ISAW measures. Centroidal frequency ML of sway deteriorates linearly (A, “linear deterioration”), while stride-velocity declines more rapidly at old age than young and middle age (B, “decline after plateau”); Black line, linear regression equation; Dashed line, 95% CI; Red and blue line, nonparametric loess line. ISAW; instrumented stand and walk test, ML; medio-lateral, CI; confidence interval.
2. 노인 비정상 보행의 특징
노인 보행은 정상적 노화 과정과 다양한 질병 등에 의해 동시에 영향을 받을 수 있으며, 정상 노인 보행에 대한 학계의 정의 또한 명확하지 않아 노인에서 나타나는 보행 변화가 정상적 노화에 따른 현상인지, 질병에 의한 결과로 나타나는 현상인지 또는 손상에 대한 보상 기전에 따른 현상인지를 명확히 구분하기는 어렵다. 그러나 최근에는 연령 증가에 따른 보행 양상의 변화를 단순히 정상적 노화에 따른 필연적인 결과로 인식하기보다는 노인 집단의 높은 질환 유병률과 질병 중증도에 의해 나타나는 현상이라는 근거가 점차 증가하고 있다[11-13]. 물론, 일부 학자들은 동반된 질환이나 신경학적 소견이 전혀 없는 노인 보행 양상, 즉 짧은 보폭과 넓은 양발 간격, 팔 흔들기의 감소, 구부정한 자세, 골반과 무릎이 굽혀진 자세, 방향 전환 시의 뻣뻣함, 드물게 발생하는 보행시작장애, 전방으로 넘어지려는 경향만을 보이는 경우 “본태성 또는 특발성 노인 보행(essential or idiopathic senile gait disorder)”으로 여전히 분류하고 있으나 이러한 보행 양상은 다른 질환의 초기 단계에서 나타날 수 있고, 점차 다른 형태의 보행장애 양상으로 변화할 수 있으며, 종종 알츠하이머 치매나 혈관성 치매에서 인지기능 저하가 진행됨에 따라 뚜렷하게 나타나는 경향을 보인다는 점에서 다양한 기저 원인 질환에 의한 병적 변화들이 투영된 결과일 가능성 또한 배제하기 어렵다[13]. 따라서, 노인의 경미한 비정상 보행을 단순히 “노인성” 보행장애(“senile” gait disorder)로 치부하기보다는 가능하면 다양한 기저 원인 질환 동반 유무에 대한 적절한 평가가 이루어져야 한다.
노인 비정상 보행을 평가하고, 진단할 때 반드시 고려해야 할 사항은 다양한 원인 질환 또는 의학적 상태가 동일한 형태의 보행 양상을 보일 수 있으므로 신경과적/비신경과적 질환, 약물 등 폭넓은 요인에 대한 광범위한 접근이 바람직하다[4,14]. 일차 의료 현장에서 흔히 보는 비정상 노인 보행의 기저 원인으로는 퇴행성 관절염, 후천성 근골격계 변형, 파행, 정형외과적 수술 후, 뇌졸중 후 장애, 기립성 저혈압 등이 있으며, 신경과에 의뢰된 환자에서는 편마비, 뇌혈관질환 또는 정상압 수두증과 같은 전두엽 보행장애, 전정 신경계 및 시신경계 이상, 척수질환, 진단되지 않은 파킨슨병 또는 파킨슨 증후군 그리고 소뇌질환 등이 흔하다[2]. 그 밖에도, 드물지만 콩팥질환 또는 간질환과 같은 대사성 질환, 중추신경계의 종양 또는 경막하 혈종, 우울증, 정신과 약물 등도 노인 보행에 영향을 줄 수 있다[15].
3. 노인 보행장애의 분류
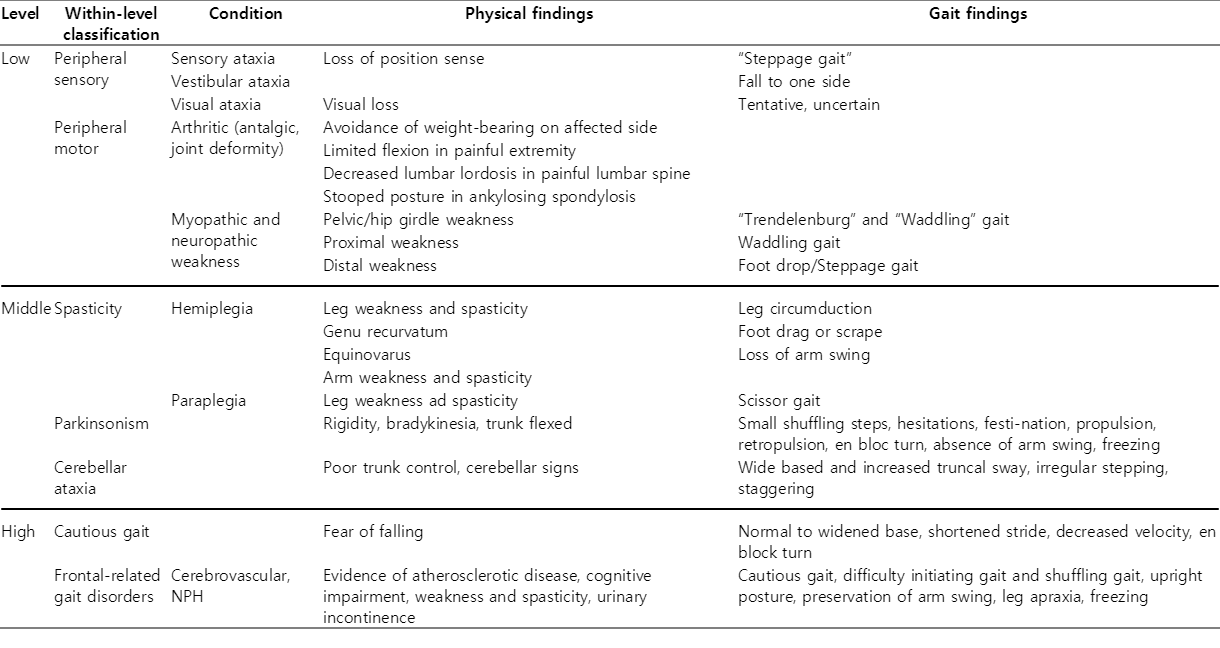
노인에서 흔히 관찰되는 보행 변화 형태는 매우 경미한 실조성/조심보행/전두엽 보행장애 양상으로 나타난다. 뚜렷한 비정상 보행의 경우 신경해부학적 범주에 따라 생리적, 계통적으로 분류해볼 수 있는데, 하위 수준(low level) 범주에는 말초감각신경 및 말초운동신경질환 그리고 근육질환이 포함되며, 중간 수준(middle level) 범주로는 중추에서 선택된 자세와 동작에 대한 실행 오류와 감각 및 운동 조정기능의 와해로 인하여 보행의 시작은 가능하지만 비정상적인 걸음을 보이는 것으로, 경직성 보행(척수질환이나 뇌졸중), 파킨슨증 그리고 소뇌질환이 포함된다. 끝으로, 상위 수준(high level) 범주는 인지기능장애가 보행장애에 비해 두드러지게 나타나는데, 치매, 우울증, 낙상에 대한 공포심 등이 해당된다(Table)[16,17]. 특히, 전두엽 보행장애(frontal-related gait disorder)는 단순한 보행개시장애만 있는 경미한 형태부터 도움 없이는 서기가 불가능한 상태의 중증 보행 이상까지 매우 광범위한 임상 양상을 보일 수 있다. 대부분의 노인 보행 이상은 노화와 동반된 다양한 기저질환에 의해 상기 범주들이 혼합된 형태로 나타나는 경우가 흔하고, 기저질환의 중등도에 따라 장애 정도에 큰 차이를 보이기도 한다.
결 론
최근까지도 노인의 정상 보행과 비정상 보행을 간명하게 객관적으로 구분하기 위한 많은 연구가 진행되고 있으나, 궁극적으로는 노화에 대한 많은 연구가 뒷받침되어야 하며, 대규모 전향적 보행 분석 연구가 필요할 것으로 생각된다.