약물과용두통: 진단기준, 역학, 치료
Medication-overuse Headache: Diagnostic Criteria, Epidemiology, and Treatment
Article information
Trans Abstract
Regular and frequent use of acute or symptomatic medications can worsen headaches and cause chronification of headache or medication-overuse headache (MOH). Although MOH is a burdensome medical condition because of disability in individual and socioeconomic aspects, difficulty in treatment, and frequent recurrence, even epidemiologic research is insufficient. Educating patients, general population, and healthcare providers about MOH is important in the first step to reducing the burden of MOH. In addition, preventing the occurrence of MOH is essential for the management of patients with a primary headache disorder. Physicians should educate and counsel the patients with MOH to stop or at least reduce the intake of acute or symptomatic medications. Withdrawal symptoms such as headache, nausea, and vomiting can be manageable with the bridging therapy using steroid or anti-emetic agents during or after the discontinuation of the overused medications. The promising efficacy of botulinum toxin A and calcitonin gene-related peptide monoclonal antibodies in the treatment of MOH have been published in the past few years. Evidencebased preventive therapies might be helpful in patients with MOH for both discontinuation of the overused medication and prevention of relapse. A comprehensive and multidisciplinary approach would improve the outcome for patients with MOH.
서 론
약물과용두통(medication-overuse headache)은 일차 두통질환을 갖고 있는 환자가 급성 또는 대증치료약물을 과용하는 경우에 발생할 수 있는 이차두통이다[1]. 편두통, 긴장형두통과 같은 일차두통질환에서의 두통발작 치료를 위한 약제를 자주 사용함으로 인해 두통발작의 강도와 빈도가 더 증가하는 악순환의 고리를 만들게 된다. 결국 의도와는 다르게, 치료가 질병(약물과용두통)의 계기가 되는 것이다.
인구집단연구에 의하면 유병률은 약 1-2% 정도로 드물지 않고[2,3], 개인 및 사회경제적으로 심각한 수준의 부정적인 영향이 알려지면서[4,5], 약물과용두통의 질병부담은 세계적인 문제로 인식되기 시작하였다. 세계보건기구의 세계질병부담연구(Global Burden of Disease)에서 장애생활연수(years-lived with disability)로 평가한 장애정도평가 결과, 약물과용두통은 1990년 23위, 2005년 22위, 2015년에는 20위로 그 질병 부담이 증가하였다[6]. 본래 만성편두통은 전 세계적으로 여섯번째로 질병부담이 큰 질환으로 분류되었지만, 2013년부터 만성편두통에 약물과용두통이 포함되면서 순위가 세 계단 상승하였다[7]. 이렇듯 약물과용두통의 질병부담은 상당하지만 이에 대한 연구나 치료는 부족하다[8].
과거에는 약물과용두통의 치료로 과용약물중단이 우선적으로 강조되었다. 하지만 약물과용두통 환자들이 갖고 있는 일차두통의 대부분은 편두통이고, 편두통의 기전에 중요한 역할을 하는 칼시토닌유전자관련펩티드(calcitonin generelated peptide, CGRP) 작용을 억제하는 항CGRP단클론 항체 치료의 편두통 예방 치료 효과가 입증되었다[9-17]. 또한, 만성편두통에 대한 갈카네주맙, 프레마네주맙, 에레누맙, 엡티네주맙의 효과를 알아보기 위한 임상시험에 참여한 대상자 중 급성기 약제를 과용하는 하위그룹분석 연구에서도 항CGRP단클론항체는 위약군에 비해 의미 있는 효과를 보였다[18-21]. 이러한 결과들을 근거로 항CGRP단클론항체는 약물과용두통 치료의 하나의 방법으로 제시되면서 진료지침의 변화가 시작되었다[22,23].
본 종설에서는 약물과용두통의 진단기준, 역학 그리고 치료에 대해 알아보고자 한다.
본 문
1. 약물과용두통 진단기준의 변천, 인과관계에서 동반 관계로
1988년 국제두통질환분류 제1판에서는 약물유발두통(drug-induced headache)이라는 명칭으로, 만성적인 약물 사용 또는 노출에 의한 두통으로 분류되었다[24]. 2004년 국제두통질환분류 제2판에서 처음으로 약물과용두통이라는 명칭이 등장하였다[25]. 이는 급성통증 조절을 위한 잦은 약제 복용의 결과로 인해 두통의 빈도가 증가하는 것을 반영하였기 때문에 이전보다는 한 단계 발전된 진단기준이라고 할 수 있다. 하지만 제2판에서는 ‘선행 원인의 발생 이후에 두통 유발/악화 및 선행 원인의 제거 후 두통 개선’의 일반적인 이차두통의 특성을 그대로 적용하여 과용약물의 중단 후 두통이 호전되어야만 약물과용두통을 진단하였다[26]. 2013년 발행된 국제두통질환분류 제3판 베타 버전에서는 약물과용 상태와 두통을 인과관계보다는 동반 상태로 간주하여, 약물과용 후 두통 악화 및 과용약물의 중단 후 두통 개선에 대한 기준을 삭제하였다[27]. 결국 약물과용두통의 진단과 동시에 일차두통에 대한 치료를 시작할 수 있게 임상진료현장에서의 실용적인 측면이 반영된 것이다. 이후 2018년 발간된 국제두통질환분류 제3판에서도 베타 버전의 약물과용두통의 정의가 유지되었다[1].
약물과용두통은 일차두통질환이 있는 환자에서 두통의 급성 또는 대증 치료로 사용될 수 있는 약물을 월 10-15일 이상, 3개월 초과하여 사용하며, 다른 두통질환으로 더 잘 설명되지 않을 때에 진단한다(Table 1) [1]. 약물과용은 약물의 종류에 따라 기준이 다르며, 트립탄, 에르고타민과 같은 편두통전문약제, 아편유사제, 복합진통제 또는 여러 계열의 약물을 사용하는 경우에는 월 10일 이상, 아세트아미노펜, 비스테로이드소염제, 아스피린 등 단순진통제를 사용하는 경우에는 월 15일 이상 복용하면 약물과용으로 진단한다(Table 1).

Diagnostic criteria of medication-overuse headache in the International Classification of Headache Disorders, 3rd edition
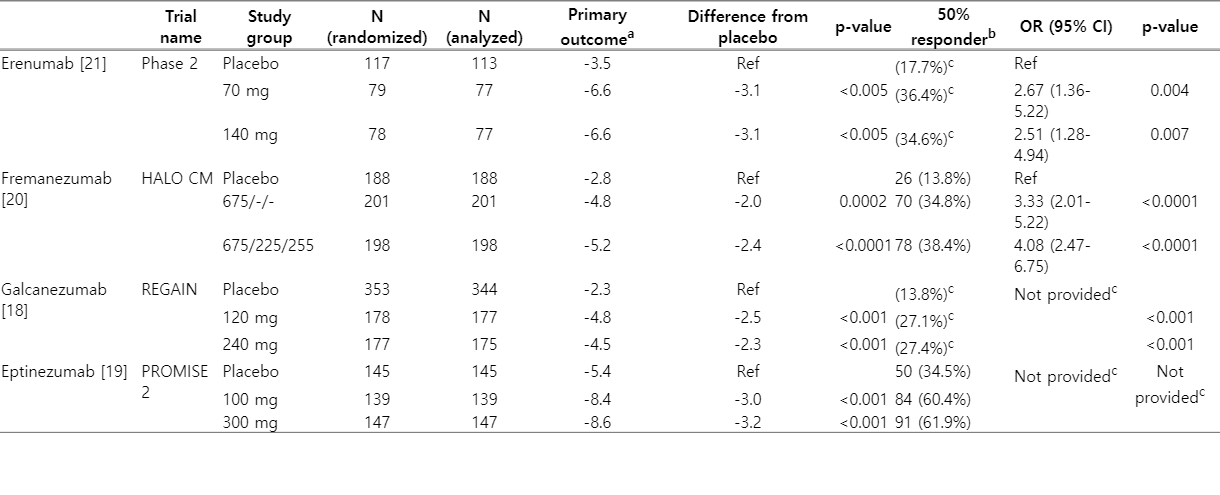
Summary of migraine preventive efficacy of CGRP monoclonal antibodies in patients with dual diagnosis of chronic migraine and medication overuse headache from the pivotal trials
2. 약물과용두통의 역학 및 특성
1) 역학
약물과용두통의 유병률은 시기적으로 적용된 진단기준과 연구마다 차이가 있긴 하지만, 일반인구집단을 대상으로 0.5-2.6%의 유병률을 갖는다고 알려져 있다[28]. 65세 이상을 대상으로 한 대만[29]과 이탈리아[30] 연구에서도 각각 1.0%, 1.7%의 유병률을 보고하였다. 만성두통 환자들을 대상으로 한 연구에서는 약물과용두통의 유병률이 11-70% 정도로 일반인구집단에 비해 매우 높다[31]. 편두통은 약물과용두통 환자들이 갖는 두통 중 가장 흔한 일차두통질환이며, 남미 연구에서는 96.6% [32], 국내 다기관 전향적 약물과용두통 레지스트리 연구(Registry for Load and Management of Medication Overuse Headache, RELEASE)에서는 99.1%가 편두통이 었다[33]. 약물과용두통을 진단받기까지 약물을 과용한 기간은 4.3-4.8년 정도였으며, 만성두통을 겪은 기간은 6.5-11년이었다[32-34]. 무작위배정대조군 연구에서는 복합진통제를 가장 흔히 과용하였으나[35], 관찰 연구들에서는 단순진통제를 가장 많이 과용하였다[32-34]. 단순진통제 다음으로는 우리나라와 유럽에서는 트립탄, 복합진통제 순이었으며, 미국에서는 복합진통제, 트립탄 순이었다[32-34].
2) 정신과적 동반질환
약물과용두통은 우울, 불안과 같은 정신과적 동반질환과 관련이 있다. 우울 정도를 측정한 방법에 따라 빈도가 다르며, 대체적으로 약물과용두통 환자의 39-83%에서 우울이 있다고 보고하였다. 미국 연구(Medication Overuse Treatment Strategy, MOTS)에 참여한 환자의 74% [34], 우리나라 연구(RELEASE)에 참여한 환자의 83% [33]에서 환자 건강설문지-9 (patient health questionnaire-9) 5점 이상인 경도 이상의 우울증이 있었다. 유럽과 남미에서 진행된 Continuous Monitoring of Medication Overuse Headache in Europe and Latin America development and Standardization of an Alert and decision support System (COMOESTAS) 연구에서는 병원불안우울척도(Hospital Anxiety and Depression Scale, HADS) 8점 이상의 우울증이 39.2%의 참여자에서 있었다[36]. 또한, MOTS 연구 및 RELEASE 연구에서는 범불안장애-7 (generalized anxiety disorder-7) 5점 이상의 경도 이상의 불안을 60% 이상 환자가 보고하였고[33,34], COMOESTAS 연구에서는 49.5%의 환자가 HADS 점수 8점 이상의 불안을 보고하였다[36]. 우울, 불안과의 선후관계에 대해서는 잘 알려져 있지 않지만, 우울과 불안이 약물과용두통의 위험과 관련이 있고[37], 약물과용을 치료하면 우울과 불안이 개선된다는 보고가 있다[38].
3. 약물과용두통의 치료
약물과용두통은 치료 이전에 발생하지 않도록 예방하는 것이 중요하다. 일차진료의, 약사, 두통 환자는 모두 급성기약제를 자주 복용하는 것이 약물과용, 약물과용두통의 발생으로 이어질 수 있음을 인지해야 한다. 따라서, 두통 빈도가 증가한다면 적절한 예방 치료를 통해 만성화를 방지하고 급성기약제를 과용하지 않도록 예방해야 한다.
약물과용두통에 대한 치료는 비약물 치료, 약물 치료로 나누어지고, 비약물 치료에는 약물중단, 인지행동 치료, 약물과용두통에 대한 교육 등이 있다. 약물 치료는 과용약물을 중단하는 초기에 흔히 발생하는 두통을 포함한 금단 증상을 개선하기 위한 연결 치료(bridging therapy) 그리고 예방 치료로 나눌 수 있다.
1) 비약물 치료
(1) 약물과용두통에 대한 교육
의료진이 약물과용두통 환자에게 과용약물 중단을 권고하고 약물과용두통에 대해 교육하는 것은 과용약물의 중단에 많은 도움을 줄 수 있다. 한 무작위배정 연구에서는 과용 약물 중단을 강력히 권고(A군), 경구스테로이드 및 예방약제 치료(B군), B군의 치료에 수액과 항구토제를 추가한 치료(C군)가 약물과용으로부터 벗어나는 것에 효과가 있는지 알아보았다(일차결과 변수: 두통 월 15일 이하 및 급성기약제 복용 10일 이내). 2개월 후 세 군 모두 양호한 치료 효과(A군 77.5%, B군 71.7%, C군 76.9%의 대상자에서 일차결과 변수에 도달)를 보였다[39]. 또한, 일차진료의가 체계적으로 단시간 교육하는 것도 치료 효과가 있었다. 약물과용두통의 위험, 급성약물 사용의 빈도 제한, 정서적 지지, 중단 시작 후 두통 악화 가능성 등에 대해 약 9분 동안 설명을 받은 군은 일상적인 진료를 받은 군에 비해 3개월 후 월두통일수가 7.3일, 급성약물사용일이 7.9일 더 감소하였고, 50%의 환자에서 삽화두통으로 개선되었다[40]. 또한, 일차진료의가 5개의 간단한 질문으로 의존성 정도를 파악하고 환자에게 공감하고 협조적인 태도를 취하는 간단한 개입만으로도 일반적인 진료 시와 비교하여 6개월째 월두통일 감소 일수 8.1일 vs. 1.9일) 및 급성약물사용일(감소 일수 11.1일 vs. 3.2일)이 크게 감소하였으며, 다시 약물과용을 하게 된 대상자는 8.3% (2/24)였다[41]. 결론적으로, 환자를 대상으로 한 교육과 조언은 약물과용두통 환자의 치료에 매우 효과적이다.
(2) 과용약물중단
약물과용두통은 급성기약제 복용을 제한하는 것만으로도 종종 삽화두통으로 바뀌기도 한다. 2000년대 초반 덴마크두통센터에서 175명의 약물과용두통 환자를 대상으로 진행한 연구에서는 과용약물을 중단하고 첫 2개월 동안은 예방치료를 하지 않았음에도 불구하고 45%는 두통 빈도가 감소하였다[42]. 2개월 동안 급성기약제를 완전히 중단하는 것과 주 2일 이내로 제한하는 것의 효과를 비교한 연구에서는 6개월 동안 추적관찰 시, 급성기약제를 완전히 중단한 군에서 월두통일 감소 비율이 유의하게 높았으며(46% vs. 22%, p=0.005), 삽화 두통으로 개선된 비율도 더 높았다(70% vs. 42%, p=0.04) [43].
과용약물은 급격하게 중단(abrupt discontinuation)할 수 있고 서서히 줄일 수도(tapering down) 있으며, 중단 기간은 보통 2주-2개월이다. 어느 방법이 더 효과적인지를 알아본 전향적 연구는 없다. 일반적으로 급격하게 중단을 하는 경우 약물중단에 의한 금단 증상 역시 빠르게 해소된다고 생각하여 많은 두통 전문가들은 급격하게 중단하는 것을 선호한다[44]. 단, 아편유사제(opioid), 바비튜르산염(barbiturate), 벤조디아제핀은 서서히 줄이는 것을 권유한다.
2) 약물 치료
약물과용두통 환자에서 진행되는 약물 치료는 크게 두 가지로 나눌 수 있다. 약물중단으로 인해 발생하는 두통을 포함한 여러 가지 증상들을 조절하기 위한 연결 치료와 약물과용두통 재발을 막고 일차두통을 조절하기 위한 예방 치료이다.
(1) 연결 치료
과용약물을 중단한 이후에 두통, 오심, 구토, 저혈압, 빈맥, 수면장애, 식욕저하, 불안, 안절부절못함 등 여러 가지 금단 증상이 발생할 수 있다[45]. 이러한 금단 증 상은 평균 3.5일 정도(2-10일) 지속되며, 트립탄을 과용한 경우(-4일)에 에르고타민(-7일)이나 일반진통제(-10일)를 과용하는 경우보다 더 짧은 경향이 있다[46,47]. 금단 증상을 조절하기 위한 치료로 연결 치료의 효과에 대해서는 여전히 논란이 있으며, 어떤 치료가 가장 좋은지는 알려져 있지 않다.
가장 흔히 사용되는 연결 치료 중 하나는 스테로이드이다. 400명의 약물과용두통 환자를 대상으로 프레드니손(2일간 60 mg 사용 후 2일마다 20 mg씩 감량)을 사용했더니 두통을 포함한 금단 증상이 감소했다는 연구 결과가 있었다[48]. 일반적인 치료를 받은 경우에 비해 5일 동안 메틸프레드니솔론 및 디아제팜을 정맥 내 투여하는 것이 3개월째 두통 빈도(9.4일 감소 vs. 3.0일 감소)와 약물 사용(19.7일 감소 vs. 6.5일 감소)을 유의하게 줄였다는 연구가 있지만[49], 다른 무작위배정 위약대조군 이중눈가림 연구에서는 약물중단 후 첫 6일 동안 경구 프레드니솔론을 사용한 것이 두통 호전에 대한 추가 효과는 없었다[50]. 비록 예비 연구(pilot study)이기는 하나 무작위배정 위약대조군 이중눈가림 연구에서 경구 프레드니손 100 mg 5일 치료군에서 위약군에 비해 첫 72시간 및 120시간 내 중등도 내지 심도의 두통이 있는 시간이 더 적었다(72시간 내 18.1시간 vs. 36.7시간, p =0.031; 120시간 내 27.2시간 vs. 42.7시간, p =0.05) [51]. 다른 무작위배정 위약대조군 이중눈가림 연구에서는 프레드니손 100 mg 5일 치료군이 위약군에 비해 일차결과 변수인 첫 3일간의 중등도 내지 심도의 두통이 있는 시간은 차이가 없었지만(20.9시간 vs. 18.2시간), 첫 5일간 구제약물 복용 빈도는 유의하게 적었다(1.1회 vs. 2.3회, p=0.021) [52]. 현재까지의 연구 결과들을 종합하면, 약물과용두통 환자에서 과용약물중단 초기의 금단 증상 및 두통을 조절하는 것에 스테로이드의 잠재적인 효과가 기대되지만, 스테로이드의 종류와 용량 등을 포함한 잘 설계된 무작위배정 위약대조군 이중눈가림 연구가 필요하다.
그 외에 수액 공급을 포함하여, 오심, 구토를 개선하기 위해 메토클로프라미드와 같은 항구토제 등을 흔히 사용한다[53]. 또한, 금단치료기에 약물과용두통 아형 중 아세트아미노펜이나 비스테로이드소염제 등 단순진통제에 의한 약물과용두통은 트립탄을, 트립탄이나 에르고타민 과용두통은 나프록센과 같이 반감기가 긴 비스테로이드소염제를 하루 2번 복용하도록 처방하는 방법도 있다.
(2) 예방 치료
약물과용두통의 기본적인 치료 단계(fundamental therapeutic step)로 예방 치료를 언급하지만[54], 예방 치료의 시작 시기에 대해서는 다양한 의견이 있다. 2020년 약물과용두통 치료 방법에 대한 체계적인 무작위배정 연구가 발표되었다. 총 120명의 약물과용두통 환자를 과용약물 중단과 동시에 예방 치료를 하는 군(A치료군), 예방 치료만 하는 군(B치료군), 과용약물 중단만 하는 군(2개월 이후에는 예방 치료 가능, C치료군)으로 1:1:1 무작위배정을 하였다. 6개월째 두통일수의 감소는 A치료군에서 12.3일, B치료군에서 9.9일, C치료군에서 8.5일이었고(p=0.20), 월편두통일수, 급성기약제의 사용, 두통강도는 의미 있는 차이가 없었다. 하지만 이차결과변수 분석에서 과용약물 중단과 예방 치료를 동시에 하는 A치료군에서 삽화두통으로의 호전이 가장 많았고(74.2% vs. B치료군 60.0% vs. C치료군 41.7%, p=0.03), 약물과용두통이 치료된 비율도 가장 높았다(96.8% vs. B치료군 74.3% vs. C치료군 88.9%, p=0.03) [35].
약제별 예방 치료의 효과 평가는 무작위배정 임상 연구의 사후분석이 대부분이며, 토피라메이트, 보툴리눔독소A, 항CGRP단클론항체에 대한 연구가 있다.
① 항CGRP단클론항체
편두통의 발생 기전에 CGRP가 매우 중요하고, 우리나라 약물과용두통 레지스트리를 이용한 RELEASE 연구에서 만성편두통이 99%를 차지하므로[33] 항CGRP단클론항체 주사제는 약물과용두통 환자에서 치료 효과가 클 것으로 기대한다. 2022년 9월 현재 우리나라에서는 갈카네주맙(Emgality®, Eli Lilly, 초기 부하용량 240 mg 후 매달 120 mg 피하주사)과 프레마네주맙(Ajovy®, Teva, 1개월마다 225 mg/3개월마다 675 mg 피하주사)을 사용할 수 있으며 갈카네주맙은 급여 기준이 신설되었다. 그 외 에레누맙(Aimovig®, Amgen/Novartis, 70/140 mg 1개월마다 피하주사)과 엡티네주맙(Vyepti®, Lundbeck, 100/300 mg 3개월마다 정맥주사)이 있으며, 엡티네주맙은 국내에서 3상 임상시험이 진행 중이다.
갈카네주맙에 대해서는 만성편두통 연구(REGAIN)에 참여한 연구 대상자 중 약물과용을 한 708명을 대상으로 한 하위그룹분석 결과가 있다[18]. 치료군에서 월편두통일이 유의하게 감소하였고(240 mg군 4.5일, 120 mg군 4.8일, 위약군 2.3일, p <0.001), 월편두통일이 50% 이상 감소한 비율도 치료군에서 높았으며(240 mg군 27.4%, 120 mg군 27.1%, 위약군 13.8%), 약물과용의 비율도 치료군에서 유의하게 감소하였다(240 mg군 47.7%, 120 mg군 47.9%, 위약군 29.6%).
프레마네주맙은 만성편두통 환자에 대한 HALO CM 연구에 포함된 1,130명 중 약물 과용이 있는 587명의 하위그룹분석 연구가 있다[20]. 치료군에서 월편두통일이 유의하게 감소하였고(분기투여군 4.8일, 월투여군 5.2일, 위약군 2.8일), 월편두통일이 50% 이상 감소한 비율도 유의하게 높았으며(분기투여군 34.8%, 월투여군 39.4%, 위약군 13.8%), 12주 연구 기간 동안 약물을 과용하는 비율도 유의하게 감소하였다(분기투여군 55.2%, 월투여군 60.6%, 위약군 46.3%).
에레누맙에 대해서는 677명의 만성편두통 환자 중 약물과용이 있는 274명을 분석하였다[21]. 다른 약제들과 마찬가지로 치료군에서 월편두통일이 유의하게 감소하였고(140 mg군 6.6일, 70 mg군 6.6일, 위약군 3.5일), 월편두통일이 50%이상 감소한 비율도 유의하게 높았으며(140 mg군 34.6%, 70 mg군 36.4%, 위약군 17.7%), 급성기편두통 약제 사용일 감소도 치료군에서 유의하게 많았다(140 mg군 4.9일, 70 mg 군 5.4일, 위약군 2.1일).
엡티네주맙은 만성편두 통 환자 를 대상으 로 진행한 PROMISE-2 연구에 포함된 환자 중 약물과용 환자를 이용한 하위그룹분석 연구가 있다[19]. 치료군에서 월편두통일이 유의하게 감소하였고(300 mg군 8.6일, 100 mg군 8.4일, 위약군 5.4일), 월편두통일이 50% 이상 감소한 비율 역시 높았다(300 mg군 61.9%, 100 mg군 60.4%, 위약군 34.5%). 연구 기간 6개월을 마친 대상자들 중에서 6개월 동안 약물과용두통 진단기준에 해당되지 않게 된 환자의 비율 역시 유의하게 높았다(300 mg군 49.5%, 100 mg군 50.5%, 위약군 27.1%).
항CGRP단클론항체는 기존에 예방 치료를 위해 사용하던 다른 약제들보다 그 효과가 빠르게 나타나며, 심지어 1-2일 이내에 효과가 나타난다는 연구 결과도 있다. 따라서 약물중단으로 인해 나타나는 두통의 발생 자체를 억제하면, 이와 관련된 금단 증상들을 빠르게 개선할 수 있을 가능성이 있다. 최근 발표된 연구에서는 만성편두통과 약물과용두통이 있고 에레누맙 또는 갈카네주맙 치료를 받은 111명의 환자에서 항CGRP단클론항체 치료 시작 전에 입원하여 과용약물을 급격하게 중단한 군(YES-DETOX)과 그렇지 않은 군(NODETOX) 을 비교하였다[55]. 3개월의 치료 후에 약물과용두통이 개선된 비율이 양 군에서 비슷하였고(56.6% vs. 64.2%, p=0.48), 월두통일수가 50% 이상 감소한 비율도 비슷하였다(50.6% vs. 53.6%, p =0.84). 따라서 항CGRP단클론항체의 시작 전에 과용약물의 감량 권고로 충분할지에 대한 추가 연구가 필요하다.
② 보툴리눔독소A
보툴리눔독소A 치료는 PREEMPT 1, 2 연구를 통해서 만성편두통에서의 예방 치료 효과가 입증되었다[56-58]. PREEMPT 1, 2 연구에 등록된 만성편두통 환자 중 약 65%에 해당하는 약물과용두통 환자들을 대상으로 통합 하위집단분석을 하였다[59]. 24주 시점에서 일차결과 변수인 보툴리눔독소A 치료군에서 월두통일(8.2일 vs. 6.2일, p <0.001), 월편두통일(8.1일 vs. 6.0일, p <0.001), 중등도 내지 심도의 두통일(7.7일 vs. 5.7일, p <0.001) 모두 유의하게 감소하였다. 월편두통일이 50% 이상 감소한 비율도 치료군에서 유의하게 높았다(47.2% vs. 33.7%, p <0.001). 3개월 또는 6개월 동안 지속적으로 약물을 과용하지 않게 된 비율도 치료군에서 유의하게 높았다(3개월 53.2% vs. 41.7%, p=0.002; 6개월 43.4% vs. 31.8%, p=0.002).
2011년 발표된 무작위배정 연구(n=68, 보툴리눔독소A vs. 위약)에서는 치료 후 12주 시점에서 일차결과 변수인 월두통일은 양 군에서 차이가 없었다(12.0 vs. 15.9, p=0.81). 하지만 급성기약물 사용일이 치료군에서 유의하게 적었다(12.1일 vs. 18.0일, p=0.03). 이 연구는 PREEMPT 연구와 비교하여 보툴리눔독소A 총 용량이 적고(155-195IU vs. 100IU), 주사부위가 적으며(31 points or more vs. 16 points), 대상자 수가 적다는 단점이 있었다[60].
최근 발표된 네덜란드 연구에서는 약물과용두통이 있는 만성편두통 환자 179명을 대상으로 급성기 약물중단 권고 및 보툴리눔독소A 치료를 무작위 배정(155단위 vs. 17.5단위. 17.5단위는 위약군에서 이마의 주름살이 개선되지 않음으로 인해 위약군임이 노출되지 않게 하기 위해 주사함)하였다. 12주 후 두통일 감소(5.6일 vs. 4.4일, p=0.17), 삽화편두통으로 개선(65.2% vs. 57%, p=0.29), 50% 이상 두통일 감소 비율(18.1% vs. 20.4%) 모두 차이가 없었다[61]. 하지만 이 연구에서의 대조군에 이마의 주름살 개선을 위해 투여한 17.5단위의 보톡스로 인해 두통일이 감소했을 가능성도 있다는 것이 단점으로 지적되었다.
③ 토피라메이트
토피라메이트를 이용한 연구는 만성편두통 환자들을 대상으로 한 이중맹검 연구이다. 토피라메이트 치료군과 위약군에 1:1로 무작위 배정하여 16주간 추적관찰하였다. 전체 환자 중 78%가 약물과용두통 진단기준에 합당하였다. 토피라메이트 치료군에서 월평균편두통일이 3.5일 감소하여 위약군(0.8일 증가)보다 유의하게 효과가 있었으며(p=0.03), 50% 이상 월편두통일이 감소한 비율도 더 많았다(29% vs. 0%, p=0.012) [62].
④ 발프로산나트륨
발프로산나트륨을 이용한 연구는 약물과용두통이 있는 편두통 환자를 대상으로 무작위배정 이중맹검 위약대조군 연구로 발프로산나트륨 800 mg과 위약을 3개월 치료 기간 동안 비교하였다. 50% 이상 두통일이 감소한 비율이 치료군에서 유의하게 높았으며(45.0% vs. 23.8%, p=0.043), 월두통일도 더 많이 감소하였고(8.1일 vs. 4.6일, p=0.012), 급성기약제 복용일도 더 많이 감소하였다(8.6일 vs. 4.9일, p=0.013) [63].
4. 재발 예방
2004년에서 2014년까지 발표된 22개의 약물과용두통 연구들을 모아서 발표한 체계적 고찰에서는 12개월 추적관찰을 하는 동안 재발률이 0-45%로 매우 다양했으며 대부분 25-35% 정도 재발하였다[64]. 정신과적 동반질환이 있는 경우, 특히 우울증은 약물과용두통 재발의 중요한 예측인자였다[65]. 알람 기능이 있는 전자 두통일기를 사용한 군에서 종이 두통일기를 사용한 군보다 약물 과용을 하지 않는 비율이 더 높았다(73% vs. 64%) [66]. 앞서 기술한 연구들에서처럼 과용약물을 중단 또는 감량하는 것이 두통을 줄일 수 있기는 하지만, 해당 환자가 기저에 갖고 있는 일차두통까지 치유할 수 있는 것은 아니다. 따라서, 일차두통을 지속적으로 관리하여 약물과용두통이 재발하지 않도록 하는 것이 반드시 필요하겠다.
결 론
약물과용두통은 높은 유병률(일반인구집단의 0.5-2.6%, 만성두통 환자의 11-70%)과 높은 질병부담을 갖는 전 세계적인 문제이다. 점차 이 질환에 대한 관심과 이해가 높아지고 있으나 진단 및 치료에 대한 정보는 여전히 부족하다. 약물과용두통은 원칙적으로는 예방할 수 있는 이차두통이며[22], 약물과용두통에 대한 인식, 환자, 일반 대중, 의료인들에 대한 교육이 매우 중요하다.
약물과용두통이 생긴 이후에는 모든 환자에게 과용약물을 중단하거나 감량하도록 권고해야 하며, 일반적으로는 약물을 급격하게 중단하는 것이 큰 문제는 없으나, 아편유사제나 바비튜르산염에 의한 약물과용두통인 경우에는 서서히 줄이는 것을 권유한다. 2주에서 2개월 동안 급성기약물을 완전히 제한할 수도 있고, 주 2회 이내로 제한할 수도 있다.
중단 자체로 약물과용두통이 상당히 호전되기는 하지만, 중단을 어려워하는 환자가 많기 때문에 기저에 갖고 있는 일차 두통질환에 대한 예방 치료가 병행되면 더 큰 치료 효과를 기대할 수 있다. 항CGRP단클론항체, 보툴리눔독소A, 토피라메이트가 두통일, 편두통일, 급성약물 사용의 감소에 효과적일 수 있으며, 질병부담의 감소에 도움이 되리라 기대한다.