기억력 저하를 호소하는 환자에서 음주 여부에 따른 인지기능 차이: 주관적인지 저하, 경도인지장애, 알츠하이머형치매 집단 비교
Impact of Current Alcohol Consumption on Cognitive Function in Patients with Self-Perceived Memory Decline: A Comparative Study of Subjective Cognitive Decline, Mild Cognitive Impairment and Alzheimer-Type Dementia Groups
Article information
Trans Abstract
Background
Alcohol consumption has been considered as a modifiable risk factor for dementia development and alcohol-related brain damage may further impair cognitive abilities in dementia patients. This study aimed to find out the differences in cognitive function according to current alcohol drinking in patients with self-perceived memory decline, including subjective cognitive decline (SCD), mild cognitive impairment (MCI) and early Alzheimer-type dementia (ATD).
Methods
From May 2018 to December 2019, retrospective chart review was performed in patients who visited CHA Bundang Medical Center for cognitive decline. A two-way analysis of variance with interaction test were used to analyze the impact of alcohol consumption on cognitive function between groups.
Results
A total of 147 patients was classified into three groups of SCD (n=30), MCI (n=53), and ATD (n=64), and each group was divided into two subgroups of alcohol users and alcohol non-users, according to the current status of alcohol consumption. Between SCD, MCI and ATD groups, scores of clock drawing test and Go/No-go test were significantly lower in current alcohol users of ATD groups compared to the SCD and MCI groups (p<0.05).
Conclusions
These results suggest that current alcohol consumption has detrimental effects especially on the frontal/executive function in early ATD patients. Considering the association between frontal/executive function and ADL, our finding suggests that cessation of alcohol intake may be a therapeutic strategy to prevent ADL deterioration in patients with ATD.
서 론
치매는 기억력과 기타 인지기능 저하로 일상활동 기능 수준에 영향을 미치며 독립적으로 일상을 유지할 수 없게 되는 질환이다. 알츠하이머병은 그중 가장 흔한 원인으로 전체 환자 중 60-70%를 차지하는 것으로 보고되고 있다[1]. 최근의 제언에 따르면 알츠하이머병(alzheimer’s disease, AD)의 진단은 병태생리적으로 입증되어야하지만[2], 임상적으로는 전형적인 알츠하이머병의 인지 및 행동 증상들이 나타나며 다른 질환이 감별 배제되면 알츠하이머형치매(alzheimer-type dementia, ATD)로 진단할 수 있다[3]. 현재는 ATD에 대한 대증약물이 사용되고 있으나 근본적인 치료제 개발을 위한 다양한 연구들이 시도되어 최근 미국 식품의약국(U.S. FOOD & DRUG ADMINISTRATION, FDA)에서 처음으로 뇌내 아밀로이드를 낮추는 약물인 아두카누맙(aducanumab)이 승인되었다[4]. 그러나 초기 단계의 환자들에서 제한적인 효능을 보여 여전히 조기 진단과 예방으로 질병의 발현과 증상 진행 속도를 늦추려는 노력이 중요하다[5].
ATD의 신경병리 경과에 영향을 줄 수 있는 위험인자들 가운데 과도한 알코올 섭취, 외상뇌손상 및 대기 오염이 대표적인 조절 가능한 위험인자로 제시되었다[6]. 특히 고령자의 인지기능과 알코올 섭취에 관한 연구에서는 알코올 섭취량에 따라 인지기능저하와 관련된다는 것이 확인되었으나[7] 여전히 알코올 섭취와 치매 발병에 대한 연구 결과는 다양하게 제시되고 있다. 과도한 알코올 섭취는 치매 위험을 증가시키지만 소량 알코올 섭취는 치매 발병 예방에 도움이 된다는 연구 결과도 보고되고 있다. 그러나 연구 대상자 개인별 신진대사와 알코올에 대한 민감성에 차이가 있고 장기적으로 심혈관질환[6]과 뇌손상, 중독 위험 등을 고려하여[8] 고령자에게 알코올 섭취를 제한하도록 권고하고 있다[9]. 알코올은 중추신경에서 산화효소를 활성화시켜 활성 산소와 세포막 손상을 유발하며[10] 중뇌 및 대뇌피질에서 신경병리 변화로 인지기능을 손상시킬 수 있다[11]. 인간 대상 실험에서 알코올 섭취가 치매에 미치는 부정적인 영향은 알코올과 관련된 뇌 부피 수축, 포도당 대사의 변화 및 신경세포 밀도의 감소, 백질과 신경 손실 등과 연관 있는데 전두엽이 많은 영향을 받는 것으로 확인되고 있다[12-14]. 18F-fluorodeoxyglucose positron emission tomography scan과 신경심리검사 상관 연구에서 만성적인 알코올 섭취가 내측 전두엽 영역의 기능을 손상시켜 조직 대사율에 영향을 미치고 전두엽기능 저하와 유의한 연관성을 가지는 것으로 확인하였다[15]. 알코올에 의한 이러한 병리 손상은 초기 ATD 환자의 병리 및 인지기능에 추가로 부정적인 영향을 미칠 것으로 예상된다. 이외, 낮은 교육 수준, 고혈압, 청각장애, 흡연, 비만, 우울증, 신체 활동 부족, 당뇨병 및 사회적 비접촉이 치매 발병에 영향을 미치는 위험 요인으로 제시하였으며 대기오염을 추가한 12가지 위험 요인을 제한하면 치매를 최대 40%까지 예방하거나 지연시킬 수 있다고 보고하였다[16].
ATD 초기에는 주로 최근 일에 대한 기억력에서 문제를 보이고 병이 진행되면서 점차 일상활동 기능을 상실하는데[17] 특히, 전두엽 집행기능은 독립적이고 목적적이며 주도적으로 개인이 지향하는 행동을 성공시킬 수 있도록 하기 때문에[18] 일상활동 능력 유지에 중요한 역할을 한다. 이전 연구에서도 정상 노인과 치매 노인에서 전두엽 집행기능이 도구일상활동(instrumental activities of daily living, IADL) 변화의 유일한 예측 인자로 나타났으며[19] 초기 치매에서 일상활동과 집행기능장애의 연관성에 대한 증거가 증가하고 있다[20].
현재까지 진행된 대부분의 알코올과 치매의 상관 연구들은 치매로 진행하는데 알코올이 미치는 영향과 인지기능저하 여부에 대해서만 논의가 되어 있어, 현재 알코올을 섭취하고 있는 ATD 환자의 세부적인 인지기능 양상에 관한 연구는 없다. 이에 본 연구자들은 주관적 인지저하(subjective cognitive decline, SCD), 경도인지장애(mild cognitive impairment, MCI)와 알츠하이머형치매(ATD) 환자의 인지기능을 현재 알코올 섭취 여부에 따라 세부 영역별로 비교 분석하여 알코올 섭취가 임상 양상에 미치는 직접적인 영향을 확인하고자 한다.
대상과 방법
1. 분석 자료
2018년 5월 15일부터 2019년 12월 31일까지 기억력 저하로 분당차병원 신경과에 방문한 환자를 대상으로 하였다. 임상 평가를 받은 환자 중 면담 당시 알코올 섭취 여부에 대한 보고가 확인되고 ATD 이외의 병(전두측두엽변성, 레비소체병, 뇌혈관 질환, 외상뇌 손상, 파킨슨병, 헌팅턴병 등)이 없는 환자로 총 196명이 확인되었다. 이중 청력과 시력 상실로 신경심리검사를 완료하지 못하거나 체질량지수(body mass index, BMI)와 당뇨병, 고지혈증, 고혈압 결측치를 가지고 있는 환자를 배제하고 총 147명의 환자를 대상으로 하였다. Subjective cognitive decline initiative (SCD-I) Working Group이 제시한 SCD 진단기준[21], Petersen의 MCI 진단기준[22], National Institute on Aging-Alzheimer’s Association workgroups에서 제안한 probable AD 진단기준[23]에 따라 환자군을 분류하였으며, 30명의 SCD 환자(알코올 섭취군 12명, 알코올 비섭취군 18명), 53명의 MCI 환자(알코올 섭취군 24명, 알코올 비섭취군 29명), 64명의 초기 ATD 환자(알코올 섭취군 29명, 알코올 비섭취군 35명)의 신경심리검사 결과를 분석하였다.
이 연구는 해당 병원의 기관윤리심의위원회(Institutional Review Board)에서 승인 받아 진행되었다(IRB 2020-10-020).
2. 신경심리 평가 측정 도구
인지기능의 평가는 서울신경심리선별종합검사-제2판(Seoul Neuropsychological Screening Battery, Second Edition, SNSB-II) [24]을 이용하였으며, Seoul Neuropsychological Screening Battery-치매판(SNSB-dementia version, SNSB-D)의 global cognitive function (GCF) 점수[25], 한국판 간이정신상태검사(Korean version of mini-mental status examination, K-MMSE) [26], 임상치매평가척도(clinical dementia rating, CDR) [27], 한국판 노인 우울척도-단축형(Koran version of the geriatric depression scale short form, SGDS-K) [28], 통괄퇴화척도(global deterioration scale, GDS) [29]를 평가하였다.
SNSB-II에서 주의집중능력은 숫자 바로 따라 외우기(digit span test-forward, DST-F)와 숫자 거꾸로 따라 외우기(digit span test-backward, DST-B), 언어능력은 한국판 보스톤 이름대기검사(Korean-Boston naming test, K-BNT), 시공간 지각 및 구성능력은 시계 그리기검사(clock drawing test, CDT)와 레이복잡도형검사(rey-osterrieth complex figure test, RCFT), 기억력은 서울 언어학습검사(seoul verbal learning test, SVLT), 전두엽 집행기능은 contrasting program과 Go/No-go test, 연상단어 구술검사(controlled oral word association, COWAT)의 유창성(fluency)검사와 한국판 색 단어 간섭검사(Korean-color word stroop test: color reading, K-CWST: CR), 숫자-기호 바꿔쓰기검사(digit symbol coding, DSC)의 점수를 선택하여 분석하였다.
3. 통계 분석
통계 분석은 IBM SPSS Statistics for Windows, version 21 (IBM Corp, Armonk, N.Y, USA)를 사용하여 진행되었다. 연구 참여자의 인구통계학, 임상 자료의 연관성 분석은 피어슨 카이제곱 검정(Pearson’s chi-square test)과 독립표본의 t 검정(independent sample student’s t-test)을 분석 시행하였다.
알코올 섭취 여부에 따른 SCD, MCI, 초기 ATD 환자의 집단간 인지기능 저하 차이를 분석하기 위해 평가 시기의 연령, 학력, 고지혈증 유무, 당뇨병 유무, 고혈압 유무, BMI 지수의 공변량을 보정하여 이원배치 분산 분석(two-way analysis of variance)을 실시하였으며 알코올 섭취에 따른 세부 인지기능 영역의 변화 추이를 확인하기 위해 교호효과 분석(interaction effect)을 시행하였다. 또한 각 인지저하 단계별 알코올 섭취 여부에 따른 집단내 인지기능 차이 분석을 위해 공분산 분석(analysis of covariance)를 실시하였다.
추가적으로 치매 발현에 영향을 줄 수 있는 요인 연령, 교육 기간, 고지혈증, 당뇨병, 고혈압, BMI, 알코올 섭취 유무가 전반적인 인지기능에 영향을 미치는지 검증하기 위해 다중회귀 분석(multiple linear regression analysis)을 실시하였다. 통계학적 유의성은 모두 유의확률 0.05 이하인 경우로 정의하였다.
결 과
1. 인구통계학적 분석
총 147명의 환자를 대상으로 알코올 섭취 유무에 따라 인구통계학 분석을 실시하였다. SCD 집단 내 알코올 섭취군 환자 12명(남성 6명, 여성 6명)의 평균 연령은 62.58±8.59세로, 교육 기간은 11.17±4.30년, BMI는 23.53±2.80 kg/m2이었다. 알코올 비섭취군 환자 18명(남성 9명, 여성 9명)의 평균 연령은 68.00±10.35세로, 교육 기간은 10.83±5.91년, BMI는 24.45±2.90 kg/m2이었다. MCI 집단 내 알코올 섭취군 환자 24명(남성 11명, 여성 13명)의 평균 연령은 68.13±9.07세로, 교육 기간은 8.54±3.72년, BMI는 24.06±2.66 kg/m2이었다. 알코올 비섭취군 환자 29명(남성 13명, 여성 16명)의 평균 연령은 69.86±9.10세로, 교육 기간은 8.83±4.55년, BMI는 24.76±2.74 kg/m2이었다. 초기 ATD 집단 내 알코올 섭취군 환자 29명(남성 16명, 여성 13명)의 평균 연령은 71.76±10.99세로, 교육 기간은 9.59±4.16년, BMI는 24.15±4.13 kg/m2이었다. 알코올 비섭취군 환자 35명(남성 16명, 여성 19명)의 평균 연령은 72.20±8.47세로, 교육 기간은 11.97±3.93년, BMI는 23.45±3.20 kg/m2 이었으며 ATD 집단 내에서 알코올 섭취군에 비해 알코올 비섭취군의 교육 기간이 더 길었다(p<0.02). 그 외, 혈관질환의 위험인자인 당뇨병, 고혈압, 고지혈증 유무는 각 군에서 유의한 차이가 없었다(Table 1).
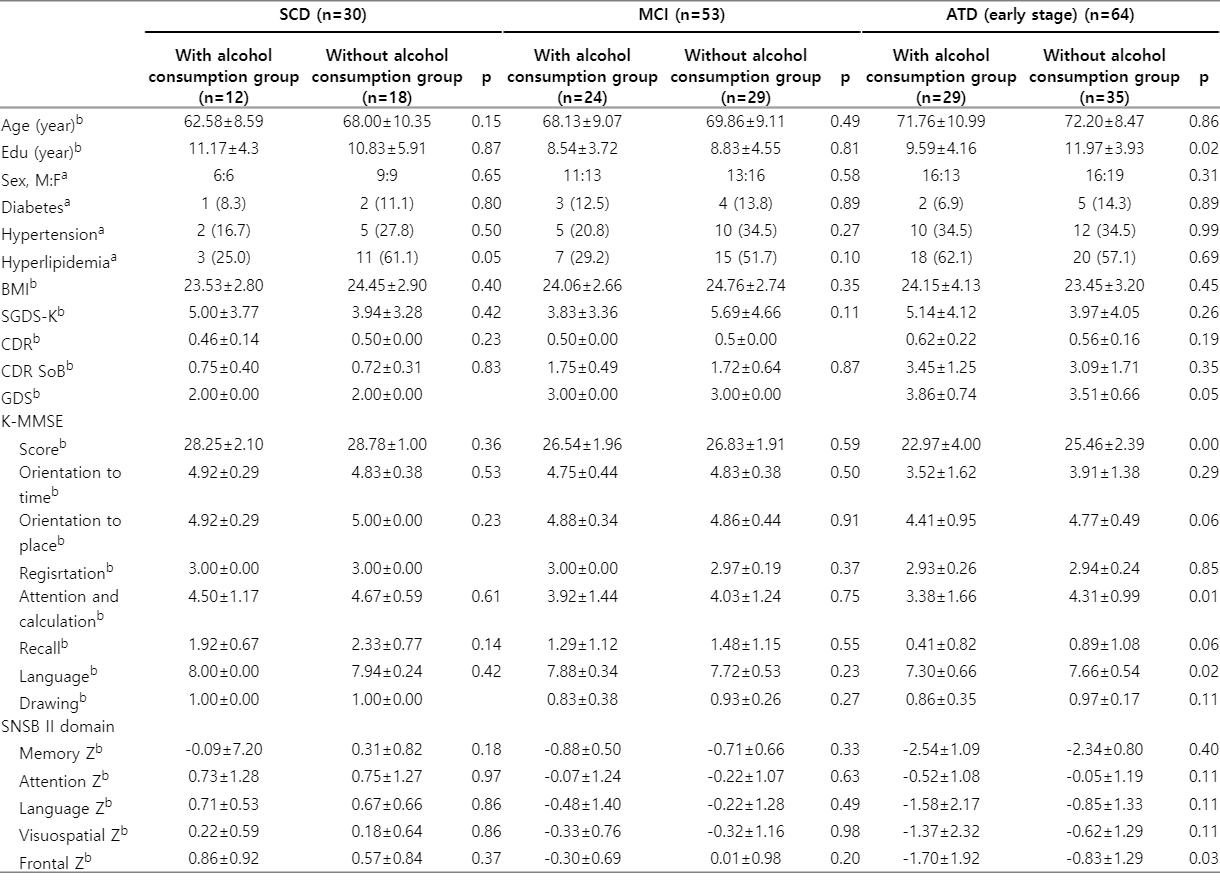
Demographic and clinical data of SCD, MCI and ATD(early stage) patients
2. SCD, MCI, 초기 ATD의 각 집단 내 알코올 섭취 여부에 따른 인지기능 차이
SCD, MCI, 초기 ATD의 집단 각각에서 알코올 섭취 여부에 따른 인지기능 차이를 분석한 결과 SCD 집단과 MCI 집단에서 각 집단 내 알코올 섭취군과 알코올 비섭취군 환자 사이에 CDR, CDR-sum of boxes, GDS, SGDS-K와 K-MMSE 총점 및 시간 지남력, 장소 지남력, 기억등록, 주의집중과 계산, 기억회상, 언어 및 시공간 구성 모두에서 유의한 차이가 나타나지 않았다. 반면, 초기 ATD 집단 내에서 K-MMSE 점수는 알코올 비섭취군에서 25.46±2.39점으로 알코올 섭취군의 22.97±4.00점에 비해 유의하게 높았다(p=0.00). 세부적으로는 K-MMSE 주의집중과 계산에서 알코올 비섭취군(4.31±0.99점)이 알코올 섭취군(3.38±1.66점)보다 평균 점수가 높았고(p=0.01) K-MMSE 언어에서도 알코올 비섭취군의 평균 점수는 7.66±0.54점으로 알코올 섭취군 7.30±0.66점보다 높아(p=0.02) 통계적으로 유의한 차이가 있었다. 교육 수준 및 연령에 따라 표준화된 SNSB-II의 각 세부 인지영역 z 점수는 SCD 집단과 MCI 집단 내 알코올 섭취군과 알코올 비섭취군에서 유의한 차이가 나타나지 않았으나, ATD 집단 내에서는 알코올 섭취군의 전두엽/집행기능 영역 점수가 -1.70±1.92점으로 알코올 비섭취군 -0.83±1.29점에 비하여 유의하게(p=0.03) 낮았다(Table 1).
연령, 교육 기간, 고지혈증 유무, 당뇨병 유무, 고혈압 유무 및 BMI 지수를 공변량으로 보정하여 SCD, MCI, 초기 ATD 집단 내 SNSB-D 총점과 SNSB-II의 각 영역별 세부검사 결과 점수를 비교하였다. SCD 집단과 MCI 집단 내 알코올 섭취군과 알코올 비섭취군에서는 모든 결과 점수에서 유의미한 차이를 보이지 않았다. 초기 ATD 집단 내에서는 알코올 섭취군과 알코올 비섭취군의 DST-F, K-BNT, RCFT Copy score, CDT, SVLT Delayed, Contrasting program, DSC 점수에서는 유의미한 차이가 나타나지 않았지만, SNSB-D 총점(p=0.00)과 DST-B (p=0.03), SVLT Recall (p=0.00), SVLT recognition (p=0.01), Go/No-go test (p=0.01), COWAT phonemic (p=0.04) 및 K-CWST: CR (p=0.02) 점수가 알코올 섭취군에서 모두 유의하게 낮게 나타났다(Table 2).
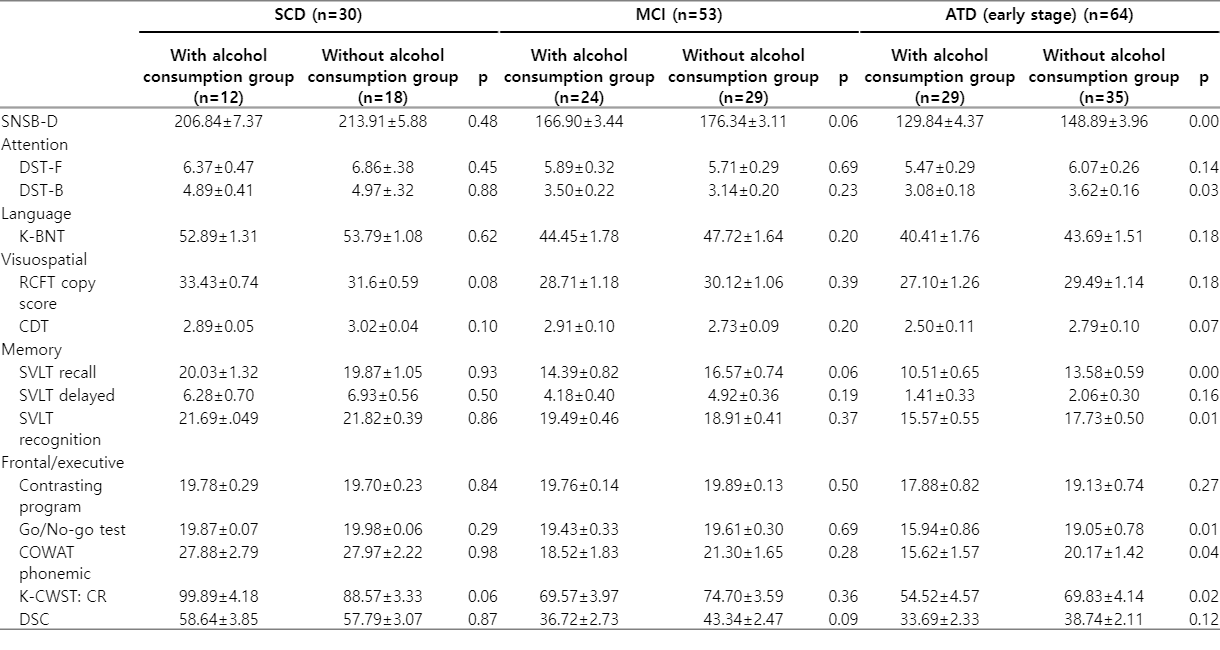
Cognitive status according to current alcohol consumption in SCD, MCI and ATD (early stage) patients
3. SCD, MCI, 초기 ATD 집단 간 알코올 섭취 여부에 따른 인지기능 저하 차이
SCD, MCI, ATD 집단 간 알코올 섭취에 따른 인지기능의 세부 영역 기능을 분석하기 위해 세 집단의 SNSB-II의 원점수(raw score)를 비교하였으며 분석 결과 SCD와 MCI 집단에 비교하여 초기 ATD 집단에서 알코올 섭취군에서 CDT (p=0.03)와 Go/No-go test (p=0.04) 점수가 더 낮게 나타났다(Table 3).

Analysis the impact of alcohol consumption on cognitive function between SCD, MCI and ATD (early stage) patients
집단 간 인지기능은 알코올 섭취 여부에 따라 통계적으로 유의한 차이가 관찰되지 않았지만, DST-F (Fig. A), DST-B (Fig. B), RCFT copy score (Fig. C), SVLT recall total score (Fig. D), SVLT recognition score (Fig. E), contrasting Program (Fig. F), COWAT phonemic total score (Fig. G), K-CWST: CR (Fig. H), DSC (Fig. I)에서 초기 ATD 환자의 인지 저하와 알코올 섭취의 교호효과(Interaction effect)가 존재할 가능성이 높을 것으로 확인되었다.
The interaction effect of cognitive decline and alcohol consumption. (A) DST-F. (B) DST-B. (C) RCFT copy score. (D) SVLT recall total score. (E) SVLT recognition score. (F) Contrasting program. (G) COWAT phonemic total score. (H) K-CWST: CR. (I) DSC. SCD; subjective cognitive decline, MCI; mild cognitive impairment, ATD; alzheimer-type dementia, DST-F; digit span test: forward, DST-B; digit span test: backward, RCFT; rey-osterrieth complex figure test, SVLT; Seoul verbal learning test, COWAT; controlled oral word association, K-CWST: CR; Korean-color word stroop test: color reading, DSC; digit symbol coding.
4. 치매 발병 위험 인자와 인지기능 세부 영역 간의 상관관계
치매 발현 위험 인자 가운데 연령, 교육 기간, 고지혈증, 당뇨병, 고혈압, BMI, 알코올 섭취 유무가 각 인지기능의 세부 영역에 미치는 영향을 검증하기 위해 다중회귀 분석을 실시하였다. 통계 분석 결과 연령(p=0.00)이나 교육 기간(p=0.00)이 높아지거나, 알코올을 섭취(p=0.02)할수록 SNSB-D 총점이 하락하는 것으로 확인되었다. 그 외, 교육 기간(p=0.00)과 당뇨병 유무(p=0.04)가 DST-F 점수에 유의한 영향을 미치고, 연령(p=0.00), 교육 기간(p=0.00), 고혈압 유무(p=0.01)는 DST-B 점수에 영향을 미치는 것으로 확인되었다. K-BNT는 연령(p=0.00), 교육 기간(p=0.01), 알코올 섭취 여부(p=0.02)에 RCFT Copy 점수는 연령(p=0.02), 교육 기간(p=0.00), 알코올 섭취 여부(p=0.04)에 영향을 받았다. 또한, SVLT Recall 점수는 연령(p=0.00), 알코올 섭취 여부(p=0.02), 고지혈증 유무(p=0.01)에, SVLT Delayed 점수와 SVLT Recognition 점수는 모두 연령(p=0.00, p=0.00)과 고지혈증 유무(p=0.01, p=0.00)가 영향을 미치는 것으로 나타났다. 알코올 사용 여부(p=0.01)는 Go/No-go test 점수에 큰 영향을 미치고 COWAT phonemic과 DSC 점수는 연령(p=0.00)과 교육 기간(p=0.00), K-CWST CR 점수는 연령(p=0.00), 교육 기간(p=0.01)이 유의한 영향을 미치는 것으로 확인되었다(Table 4).

Identifying explanatory variables to predict the cognitive outcome of alcohol consumption
고 찰
AD는 진행성 신경퇴행질환으로 임상적으로는 인지기능과 일상활동 능력의 점진적 저하와 병리적으로는 신경 위축, 시냅스 손실 및 노년판(senile plaques)의 아밀로이드-단백질 및 신경원섬유매듭으로 과인산화된 타우단백질의 비정상 축적을 특징으로 한다[30]. 알코올 섭취 과거력 및 현재 섭취량에 따라 치매 환자군을 나누어 MMSE를 분석한 선행 연구에서는 AD 발병 후 지속적으로 알코올을 섭취했지만 연구 이후 금주를 한 환자군의 인지기능은 알코올 섭취 과거력이 없는 AD 환자에 비하여 더 적게 저하되었다. 하지만 과거 고용량의 알코올 섭취를 한 집단에서는 금주효과가 없었다[31]. 이처럼 과거 알코올 섭취하였지만 그 양이 많지 않고 AD 발병 후 금주를 한다면 급격한 인지기능 저하를 예방할 수 있을 것이라고 예상된다. 또한 과도한 음주를 하지 않지만 알코올을 지속적으로 섭취하는 MCI 환자군의 인지기능 저하가 알코올 비섭취 환자군에 비해 크다는 것이 제시되었다[32]. 추적 연구에 따르면 MCI 진단 후 2-5년 이내에 치매로 진행할 가능성이 높으므로 치매 발병 여부를 유의 깊게 살펴야 하는 단계이다[33-35]. SCD는 주관적인 기억장애를 호소하지만 인지기능검사 결과가 정상인 단계로 기억장애를 호소하지 않는 정상 인지군에 비해서 알츠하이머병 발병 위험이 2배 높다고 알려져 MCI와 같이 ATD 발생 고 위험군이라는 주장이 있다[21]. ATD의 예방 및 조기 발견을 위해서는 환자의 SCD 단계에서부터 MCI와 ATD 집단의 인지기능 수준 변화의 과정을 이해하는 것이 중요할 것이다.
이 연구에서는 인지 저하의 여러 단계에서 임상적 평가 시행 시점 알코올 섭취 유무와 세부 인지영역 사이의 연관성에 대해 분석하였다. 현재 섭취하고 있는 알코올의 부정적인 효과를 포함한 인지기능 수준을 알아보기 위해 임상 평가 당시 알코올을 섭취하고 있는 환자를 포함하여 연구를 실시하였다. 또한 알코올이 주로 치매 환자의 전두엽에 부정적인 영향을 미친다는 연구 결과에 따라[12] 상대적으로 전두엽 손상이 적은 초기 ATD 환자와 SCD, MCI 환자에서 연령과 학력을 통제한 신경심리검사 결과를 포함하여 비교, 분석하였다.
통상적으로 초기 ATD 환자는 기억력 저하가 두드러지는데 알코올 섭취에 따른 SCD, MCI, ATD 집단 간 인지기능 세부 영역을 비교한 결과 알코올 섭취군의 ATD 환자는 시공간 지각 및 구성 능력 검사인 CDT와 전두엽 기능검사인 Go/No-go test에서 유의한 기능 저하를 나타냈다. CDT 검사는 시공간 지각 및 구성 능력과 함께 언어 이해력과 기억력을 필요로 하며 중증도 치매 감별이나 인지기능 저하에 효과적인 변별력이 있으나 초기 ATD 환자는 큰 오류를 보이지 않는다[36]. 그러나 알코올 관련 치매 환자 그룹은 알츠하이머병 환자 그룹보다 시공간 지각 및 구성 능력이 더 저하를 보이며 기억 및 고차원적인 집행기능과 시공간 기능 작업에서 취약한 결과가 나타난다[37]. 최근 중년과 노년을 대상으로 한 다른 연구에서도 소량의 알코올 섭취를 하는 경우 전반적인 인지기능과 단어 기억과 어휘력이 더 저하되는 것으로 보고 하였다[38]. 전두엽 기능 평가 중 Go/No-go test는 운동 조절 기능 능력에 관여하는 억제력과 인지 전환 능력을 평가할 수 있으며 충동을 조절하는 반응을 측정할 수 있다[39]. 이러한 인지기능 저하 양상은 알코올 섭취한 ATD 환자에서 기억력 저하와 동시에 시공간 지각 및 구성 능력과 전두엽 집행기능이 더 손상되고 있음을 시사하며, 알코올을 섭취하지 않는 ATD 환자의 인지 저하와 다른 결과이다. 즉, 이 연구에서는 가설과 같이 지속적으로 알코올을 섭취하는 ATD 환자군에서 기억력과 함께 다른 인지기능저하가 알코올 섭취하지 않는 ATD 환자군보다 더 크게 나타났고 알코올 섭취는 특히 전두엽 기능 저하와 관련 있는 것이 확인되었다. 이전 연구에서 집행기능의 하위 구성 요소로 인지적 유연성, 추상적 사고, 창의성, 계획능력, 통찰력, 자발성, 억제능력, 적응적인 정서, 성격과 사회적 행동이 매우 중요하며, 이러한 구성 요소의 기능은 주의력, 언어능력, 시공간 기능, 기억력에 뚜렷한 영향을 끼치고[40], 집행기능장애가 경도인지장애와 알츠하이머병 환자의 도구 일상활동 수행능력 저하에 주요 원인임이 제시되어 왔다[41]. ATD 환자도 독립적이고 자주적인 일상생활과 사회생활을 유지하는 데 중요한 역할을 하는 집행기능이 손상되지 않도록 예방하는 것이 삶의 질을 유지하는데 중요한 핵심요소이다.
본 연구 결과 알코올 섭취여부는 SCD와 MCI, ATD 집단간 비교에서 ATD 환자의 주의집중능력, 언어능력, 기억력에 유의한 영향을 끼치지 않았다. 이것은 연구에 참여한 대상자의 알코올 섭취량이 확인되지 않아 제한점이 있지만 과거 및 현재의 알코올 섭취량에 따른 차이로 인한 것으로 고려된다. 또는 SCD 집단과 MCI 집단의 비교에서 동일 대상자의 요인 대조 연구가 아니라는 점과 연관되었을 가능성이 있는데 추후에 이를 검증하기 위한 동일한 환자를 대상으로 한 추적 코호트 연구가 필요할 것이다.
이 연구의 제한점으로 알코올 섭취 유무를 자가 또는 보호자 보고에 의존하였고, 면담 당시 알코올 섭취 여부만을 확인하여, 과거 알코올 섭취 여부 및 섭취하는 알코올이 자세히 파악되지 않아 알코올 양에 따른 인지기능 저하를 분석할 수 없었다. 알코올은 섭취량, 패턴 및 빈도, 알코올의 종류, 개인의 영양 상태 및 인간 유전형에 따른 차이가 크기 때문에 알코올 섭취에 따른 ATD의 인지기능 저하에 대한 관계 및 병태생리 기전을 설명하기는 쉽지 않다[42]. 그럼에도 불구하고 본 연구를 통해 ATD 환자가 알코올 섭취를 지속하는 것과 시공간 지각 및 구성 능력과 전두엽 집행기능 저하에 미치는 연관성이 확인되었다. 또한 신경병리적 손상으로 인한 인지기능과 일상활동 저하를 예방하기 위해 초기 ATD환자의 알코올 섭취를 제한하는 치료와 관리 계획에 도움이 될 것이라는 점에이 연구의 의의가 있다.